You might also like
- History: Symptoms Associated With Specific Viral InfectionsDocument12 pagesHistory: Symptoms Associated With Specific Viral InfectionsFatima Love Ariate-ArcasetasNo ratings yet
- Central Nervous System Infections: Gonzalo B. Roman JR.,MD.,FPSPDocument72 pagesCentral Nervous System Infections: Gonzalo B. Roman JR.,MD.,FPSPBenjamin PrabhuNo ratings yet
- Hydrocephalus, (Fluid in Brain) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHydrocephalus, (Fluid in Brain) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Cns InfectionsDocument141 pagesCns InfectionsReda AlyNo ratings yet
- Hassan Tonic - Clonic SeizureDocument12 pagesHassan Tonic - Clonic SeizureHassan.shehri100% (1)
- Post Trauma EpilepsyDocument42 pagesPost Trauma Epilepsyminerva_fowlNo ratings yet
- HEMOLYSISDocument2 pagesHEMOLYSISchandra-vinnakotaNo ratings yet
- Movement Disorders BabcockDocument19 pagesMovement Disorders BabcockBaiq Trisna SatrianaNo ratings yet
- Herpes Zoster: Nurul Iska Ulmarika Idrisc111 10 831 Ruth Faustine J. Rayo C 1 1 1 1 0 1 8 0Document26 pagesHerpes Zoster: Nurul Iska Ulmarika Idrisc111 10 831 Ruth Faustine J. Rayo C 1 1 1 1 0 1 8 0fatqur280% (1)
- Rosalina Q. de Sagun, M.D. Maria Antonia Aurora Moral - Valencia, M.DDocument52 pagesRosalina Q. de Sagun, M.D. Maria Antonia Aurora Moral - Valencia, M.DDaphne Jo ValmonteNo ratings yet
- Systemic Lupus ErythematosusDocument51 pagesSystemic Lupus ErythematosusEmma AndayaNo ratings yet
- Understanding Encephalitis: Causes, Symptoms and TreatmentDocument104 pagesUnderstanding Encephalitis: Causes, Symptoms and TreatmentAsogaa MeteranNo ratings yet
- Amyotrophic Lateral SclerosisDocument23 pagesAmyotrophic Lateral SclerosisAfshan Pt T100% (1)
- Head InjuryDocument50 pagesHead InjuryThiagarajah RaviNo ratings yet
- Rare Muscle Diseases: PM and DMDocument2 pagesRare Muscle Diseases: PM and DMintrovoyz041No ratings yet
- Head Injury 2Document47 pagesHead Injury 2drvishal bhattNo ratings yet
- Encephalitis Causes, Symptoms & DiagnosisDocument55 pagesEncephalitis Causes, Symptoms & DiagnosisAmit MartinNo ratings yet
- Amyotrophic Lateral SclerosisDocument58 pagesAmyotrophic Lateral SclerosisAathi PathmanathanNo ratings yet
- Meningitis Pathophysiology PDFDocument59 pagesMeningitis Pathophysiology PDFpaswordnyalupa100% (1)
- Cerebellar DisordersDocument51 pagesCerebellar DisorderswasimNo ratings yet
- Acute Lymphoblastic LeukemiaDocument22 pagesAcute Lymphoblastic Leukemiaحسن محمدNo ratings yet
- 0812 Hypoxic Ischemic Encephalopathy PDFDocument35 pages0812 Hypoxic Ischemic Encephalopathy PDFPutriNo ratings yet
- Bipolar 1Document43 pagesBipolar 1rtishaiiNo ratings yet
- Management MastitisDocument6 pagesManagement MastitisReza Hardian NatsirNo ratings yet
- Childhood Seizure DisordersDocument57 pagesChildhood Seizure DisordersashuNo ratings yet
- CNS Infection 11Document75 pagesCNS Infection 11Paulo Josue SabladNo ratings yet
- Tourette'S Disorder: Presented byDocument14 pagesTourette'S Disorder: Presented byjaydipNo ratings yet
- Tuberculosis Power PointDocument20 pagesTuberculosis Power PointLeena LapenaNo ratings yet
- EncephalitisDocument30 pagesEncephalitisHITIPHYSIO100% (1)
- RP-Case History of A Child With Sickle Cell Anemia in IndiaDocument5 pagesRP-Case History of A Child With Sickle Cell Anemia in IndiaMarie Kelsey Acena MacaraigNo ratings yet
- Neonatal Hypoxic Ischemic Encephalopathy-Related Biomarkers in Serum and 2015 PDFDocument63 pagesNeonatal Hypoxic Ischemic Encephalopathy-Related Biomarkers in Serum and 2015 PDFVanessa CruzNo ratings yet
- Tenofovir Disoproxil Fumarate: Therese M. Chapman, Jane K. Mcgavin and Stuart NobleDocument12 pagesTenofovir Disoproxil Fumarate: Therese M. Chapman, Jane K. Mcgavin and Stuart NobleBagusHibridaNo ratings yet
- Antiphospholipid Antibody Syndrome and PregnancyDocument17 pagesAntiphospholipid Antibody Syndrome and Pregnancybidan22No ratings yet
- Neuroleptic Malignant SyndromeDocument18 pagesNeuroleptic Malignant Syndromedrkadiyala2No ratings yet
- Disorders of Hemoglobin Structure and ThalassemiasDocument10 pagesDisorders of Hemoglobin Structure and ThalassemiasManisanthosh KumarNo ratings yet
- Anticancer Drugs: Pharmacology 2Document74 pagesAnticancer Drugs: Pharmacology 2Hannah Laput100% (1)
- Nephrotic Syndrome 2016Document45 pagesNephrotic Syndrome 2016alaaNo ratings yet
- L AsparaginaseDocument2 pagesL AsparaginaseBigBoostingNo ratings yet
- Nervous System PathologyDocument57 pagesNervous System Pathologypatriciasuscking100% (1)
- Tuberculous Meningitis Diagnosis, Treatment and Impact of HIVDocument34 pagesTuberculous Meningitis Diagnosis, Treatment and Impact of HIVLuvi PujiNo ratings yet
- Acute CNS Infections Diagnosis GuideDocument53 pagesAcute CNS Infections Diagnosis GuideEhab KhiryNo ratings yet
- Pathophysiology of Bacterial MeningitisDocument2 pagesPathophysiology of Bacterial MeningitisEvangel PaduaNo ratings yet
- Drug DilantinDocument1 pageDrug DilantinSrkocherNo ratings yet
- Antiepileptics (Autosaved)Document57 pagesAntiepileptics (Autosaved)vishal singhNo ratings yet
- Pharmacology Neurotropic Drugs 2015Document44 pagesPharmacology Neurotropic Drugs 2015Migz BrosasNo ratings yet
- Cerebrovascular AccidentDocument79 pagesCerebrovascular AccidentKathy B. AbuanNo ratings yet
- CretinismDocument15 pagesCretinismJoshua fuentesNo ratings yet
- Myasthenia Gravis PathophysiologyDocument2 pagesMyasthenia Gravis PathophysiologyRyan Daet0% (1)
- Hypertensive RetinopathyDocument27 pagesHypertensive RetinopathyChikita Artia SariNo ratings yet
- Meconium Aspiration Syndrome: Walter Otieno Consultant PaediatricianDocument27 pagesMeconium Aspiration Syndrome: Walter Otieno Consultant PaediatricianMalueth AnguiNo ratings yet
- NTB Control Program ObjectivesDocument46 pagesNTB Control Program ObjectivesJai AdoraNo ratings yet
- 2-Sickle Cell Anemia PDFDocument21 pages2-Sickle Cell Anemia PDFJennyu YuNo ratings yet
- Cyclosporine Clinical Uses, Dosage, Monitoring & InteractionsDocument24 pagesCyclosporine Clinical Uses, Dosage, Monitoring & Interactionssanchit_J14No ratings yet
- Thalassemia Case StudyDocument13 pagesThalassemia Case StudyNellyWataNo ratings yet
- Endometriosis: Causes, Symptoms and TreatmentDocument31 pagesEndometriosis: Causes, Symptoms and TreatmentChauthiran Agamudaiyar100% (1)
- 2.11 SEPTIC ABORTION AND SEPTIC SHOCK. M. Botes PDFDocument4 pages2.11 SEPTIC ABORTION AND SEPTIC SHOCK. M. Botes PDFteteh_thikeuNo ratings yet
- REYE SYNDROME: ACUTE ENCEPHALOPATHY AND FATTY LIVERDocument10 pagesREYE SYNDROME: ACUTE ENCEPHALOPATHY AND FATTY LIVERDanil KhairulNo ratings yet
- Fluanxol Depot: Name of MedicineDocument11 pagesFluanxol Depot: Name of MedicineIvo_NichtNo ratings yet
- Booking details for Bhubaneswar to New Delhi flightsDocument2 pagesBooking details for Bhubaneswar to New Delhi flightsPrateek Kumar PandaNo ratings yet
- JHGDocument2 pagesJHGPrateek Kumar PandaNo ratings yet
- Understanding Intelligence TestsDocument20 pagesUnderstanding Intelligence Testsharpreet100% (2)
- DM Teaching Roster For Month of December 2020, Department of Paediatrics Date Day Activity Topic Presenter ModeratorDocument1 pageDM Teaching Roster For Month of December 2020, Department of Paediatrics Date Day Activity Topic Presenter ModeratorPrateek Kumar PandaNo ratings yet
- Stippled Epiphyses in The Newborn and in Infants (Synonyms: Chondrodystrophia Calcificans Congenita, Dysplasia Epiphysialis Punctata)Document18 pagesStippled Epiphyses in The Newborn and in Infants (Synonyms: Chondrodystrophia Calcificans Congenita, Dysplasia Epiphysialis Punctata)Prateek Kumar PandaNo ratings yet
- Intracranial Hemangiomas Cause Childhood Temporal Lobe EpilepsyDocument2 pagesIntracranial Hemangiomas Cause Childhood Temporal Lobe EpilepsyPrateek Kumar PandaNo ratings yet
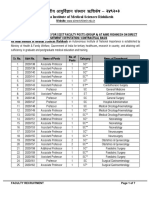
- Faculty SRD Advt - 2020 - 138-168 - SC - STDocument7 pagesFaculty SRD Advt - 2020 - 138-168 - SC - STPrateek Kumar PandaNo ratings yet
- Prof Sheffali Gulati: MD, Fiap, FimsaDocument3 pagesProf Sheffali Gulati: MD, Fiap, FimsaPrateek Kumar PandaNo ratings yet
- Pediatric Neuromuscular Diseases Update Webinar SeriesDocument4 pagesPediatric Neuromuscular Diseases Update Webinar SeriesPrateek Kumar PandaNo ratings yet
- Definitions - Neuroanatomical Basis - Clinical Approach - Diagnosis - Management - Case VignetteDocument5 pagesDefinitions - Neuroanatomical Basis - Clinical Approach - Diagnosis - Management - Case VignettePrateek Kumar PandaNo ratings yet
- 32 IndianDocument3 pages32 IndianPrateek Kumar PandaNo ratings yet
- Neurofibromatosis Type I: Spinal Neoplasia Without SymptomsDocument3 pagesNeurofibromatosis Type I: Spinal Neoplasia Without SymptomsPrateek Kumar PandaNo ratings yet
- 4 Non IndexedDocument8 pages4 Non IndexedPrateek Kumar PandaNo ratings yet
- Assent Induction EnglishDocument2 pagesAssent Induction EnglishPrateek Kumar PandaNo ratings yet
- Autoimmune EncephalitisDocument43 pagesAutoimmune EncephalitisPrateek Kumar PandaNo ratings yet
- Basal Ganglia TableDocument1 pageBasal Ganglia TablePrateek Kumar PandaNo ratings yet
- Status Final SlidesDocument19 pagesStatus Final SlidesPrateek Kumar PandaNo ratings yet
- 10 DecDocument10 pages10 DecPrateek Kumar PandaNo ratings yet
- Picf Autism English PDFDocument1 pagePicf Autism English PDFPrateek Kumar PandaNo ratings yet
- PredictionDocument13 pagesPredictionPrateek Kumar PandaNo ratings yet
- NMJDocument22 pagesNMJPrateek Kumar PandaNo ratings yet
- Picf Dystrophy English PDFDocument1 pagePicf Dystrophy English PDFPrateek Kumar PandaNo ratings yet
- Answer To The CommentsDocument1 pageAnswer To The CommentsPrateek Kumar PandaNo ratings yet
- Novak2013 PDFDocument26 pagesNovak2013 PDFRifa YulitaNo ratings yet
- Assent Induction EnglishDocument2 pagesAssent Induction EnglishPrateek Kumar PandaNo ratings yet
- Air PollutionDocument6 pagesAir PollutionPrateek Kumar PandaNo ratings yet
- Article 4 NL RatioDocument4 pagesArticle 4 NL RatioPrateek Kumar PandaNo ratings yet
- Epilepsy and Attention-Deficit Hyperactivity Disorder: Links, Risks, and ChallengesDocument10 pagesEpilepsy and Attention-Deficit Hyperactivity Disorder: Links, Risks, and ChallengesPrateek Kumar PandaNo ratings yet
- Autism Pathogenesis 2Document18 pagesAutism Pathogenesis 2Prateek Kumar PandaNo ratings yet
- Medicalization of Racial Features Asian American Women and Cosmetic SurgeryDocument17 pagesMedicalization of Racial Features Asian American Women and Cosmetic SurgeryMadalina ElenaNo ratings yet
- Book Review Reclaim Your HeartDocument7 pagesBook Review Reclaim Your HeartShaheer KhanNo ratings yet
- Bombardier CityfloDocument14 pagesBombardier CityfloBiju KmNo ratings yet
- Universitas Alumni Psikotest LolosDocument11 pagesUniversitas Alumni Psikotest LolosPsikotes BVKNo ratings yet
- My Perspective On Ayurveda-ArticleDocument2 pagesMy Perspective On Ayurveda-ArticleAaryan ParashuramiNo ratings yet
- Ad844 PDFDocument20 pagesAd844 PDFkavi_mishra92No ratings yet
- Functional Appliances 2018Document45 pagesFunctional Appliances 2018tonhanrhmNo ratings yet
- Philhis Handouts Week 1Document5 pagesPhilhis Handouts Week 1Jeen JeenNo ratings yet
- Logic Puzzles Freebie: Includes Instructions!Document12 pagesLogic Puzzles Freebie: Includes Instructions!api-507836868No ratings yet
- Phantom Susan KayDocument379 pagesPhantom Susan Kaytheeyeofthemoon100% (9)
- Twin-Field Quantum Key Distribution Without Optical Frequency DisseminationDocument8 pagesTwin-Field Quantum Key Distribution Without Optical Frequency DisseminationHareesh PanakkalNo ratings yet
- ViscosityDocument7 pagesViscositykiran2381No ratings yet
- What's The Line Between Middle Class, Upper Middle Class, and Upper Class in Britain - QuoraDocument11 pagesWhat's The Line Between Middle Class, Upper Middle Class, and Upper Class in Britain - QuoraFaizan ButtNo ratings yet
- Apostles CreedDocument141 pagesApostles Creedjerome mecca0% (2)
- Crypto Portfolio Performance and Market AnalysisDocument12 pagesCrypto Portfolio Performance and Market AnalysisWaseem Ahmed DawoodNo ratings yet
- The Human Element is Critical in Personal SellingDocument18 pagesThe Human Element is Critical in Personal SellingArsalan AhmedNo ratings yet
- New Text DocumentDocument8 pagesNew Text DocumentDhaniNo ratings yet
- Intrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Document12 pagesIntrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Roy MontoyaNo ratings yet
- Ch.24.2 Animal Evolution and DiversityDocument34 pagesCh.24.2 Animal Evolution and DiversityweldeenytNo ratings yet
- PIC16 F 1619Document594 pagesPIC16 F 1619Francisco Martinez AlemanNo ratings yet
- Tle-Bpp 8-Q1-M18Document14 pagesTle-Bpp 8-Q1-M18Michelle LlanesNo ratings yet
- Connectors/Conjunctions: Intermediate English GrammarDocument9 pagesConnectors/Conjunctions: Intermediate English GrammarExe Nif EnsteinNo ratings yet
- SDLC - Agile ModelDocument3 pagesSDLC - Agile ModelMuhammad AkramNo ratings yet
- Role of TaxationDocument5 pagesRole of TaxationCarlo Francis Palma100% (1)
- Louis Theroux PowerpointDocument6 pagesLouis Theroux Powerpointapi-330762792No ratings yet
- People v. Cresencia ReyesDocument7 pagesPeople v. Cresencia ReyesAnggling DecolongonNo ratings yet
- Why Narcissists Need You To Feel Bad About Yourself - Psychology TodayDocument51 pagesWhy Narcissists Need You To Feel Bad About Yourself - Psychology Todaytigerlo75No ratings yet
- 59-33 ATO Implementation Journal KSA 100Document18 pages59-33 ATO Implementation Journal KSA 100nicolas valentinNo ratings yet
- 5 - Econ - Advanced Economic Theory (Eng)Document1 page5 - Econ - Advanced Economic Theory (Eng)David JackNo ratings yet
- Christian Appraisal of Feminist Ideologies Among Nigerian Women 2020Document78 pagesChristian Appraisal of Feminist Ideologies Among Nigerian Women 2020Nwaozuru JOHNMAJOR ChinecheremNo ratings yet