You might also like
- Congestive Cardiac FailureDocument39 pagesCongestive Cardiac Failurezacks nyirongoNo ratings yet
- Drugs For Congestive Heart FailureDocument46 pagesDrugs For Congestive Heart Failuresultan khabeeb100% (1)
- Congestive Heart FailureDocument25 pagesCongestive Heart Failureemman122392No ratings yet
- Chapter 2 - A - III Hypertension TreatmentDocument37 pagesChapter 2 - A - III Hypertension TreatmentEmmaNo ratings yet
- CHF 5Document2 pagesCHF 5Agus HaryantoNo ratings yet
- CVS PharmacologyDocument60 pagesCVS PharmacologyGølà Sèèñàà–baale irraaNo ratings yet
- PharmaDocument8 pagesPharma2022105340No ratings yet
- Cad CommerDocument2 pagesCad CommerWhatDoYouSeriesNo ratings yet
- Congestive Heart Failure: Dr. J. SaravananDocument31 pagesCongestive Heart Failure: Dr. J. Saravananpetervazhayil100% (1)
- Study Guide For Final Pharmacology HypertensionDocument39 pagesStudy Guide For Final Pharmacology HypertensionAlejandro Daniel Landa MoralesNo ratings yet
- Pulmonary Edema by DR Gireesh Kumar K PDocument16 pagesPulmonary Edema by DR Gireesh Kumar K PAETCM Emergency medicineNo ratings yet
- عرض تقديمي2Document18 pagesعرض تقديمي2Sabrina ShalhoutNo ratings yet
- Farmakologi 1 Antihypertension: NURUL HASANAH (1800085)Document31 pagesFarmakologi 1 Antihypertension: NURUL HASANAH (1800085)MutiaraBintangNo ratings yet
- Pharmacology 3Document7 pagesPharmacology 3Maria Nichole JavarNo ratings yet
- HTN JmiDocument39 pagesHTN Jmink999999No ratings yet
- Cardiotronic MedicationsDocument13 pagesCardiotronic MedicationsTee WoodNo ratings yet
- Pharmacology 3 - Management of Heart FailureDocument59 pagesPharmacology 3 - Management of Heart Failurealbatros000No ratings yet
- HEART FAILURE Dr. Samira BelkheirDocument46 pagesHEART FAILURE Dr. Samira BelkheirkalfNo ratings yet
- Pharmacology Chapter 42 p-3Document19 pagesPharmacology Chapter 42 p-3sho bartNo ratings yet
- Cardiac DrugsDocument35 pagesCardiac DrugsCristina Centurion100% (3)
- Emergency Drugs Review: Oxygen, Epinephrine, Atropine and MoreDocument71 pagesEmergency Drugs Review: Oxygen, Epinephrine, Atropine and Moredodong skyroseNo ratings yet
- SEC A GP 1 OsamaDocument16 pagesSEC A GP 1 OsamaAiman SiddiquiNo ratings yet
- Drugs Used in Cardio Vascular SystemDocument138 pagesDrugs Used in Cardio Vascular SystemSagun lohalaNo ratings yet
- 1 Drugs For HypertensionDocument62 pages1 Drugs For HypertensionSaniNo ratings yet
- Chaper 20 Study CardsDocument8 pagesChaper 20 Study Cardsheldai1No ratings yet
- Heart FailureDocument28 pagesHeart FailureaparnaNo ratings yet
- Antihypertensive DrugsDocument37 pagesAntihypertensive Drugsleiann_jessicaNo ratings yet
- Cardiac MedsDocument10 pagesCardiac MedsSareeta MarieNo ratings yet
- Cardiovascular Agents: Florianne E. Adlawan, R.NDocument31 pagesCardiovascular Agents: Florianne E. Adlawan, R.NadlawanflorianneNo ratings yet
- Chapter 37 Cardiac Glycosides Antianginals and AntidysrhythmicsDocument5 pagesChapter 37 Cardiac Glycosides Antianginals and AntidysrhythmicsErika Joy Cabison TamayoNo ratings yet
- Oral Anti-HTN Medications: ACE Inhibitors, ARBs, CCBs, Diuretics, Beta BlockersDocument84 pagesOral Anti-HTN Medications: ACE Inhibitors, ARBs, CCBs, Diuretics, Beta Blockersأبوأحمد الحكيمNo ratings yet
- Captopril Pharmacological Properties and UsesDocument13 pagesCaptopril Pharmacological Properties and UsesputrinadNo ratings yet
- Heart Failure Dr. VishvasDocument31 pagesHeart Failure Dr. VishvasvishvasNo ratings yet
- Hypertension: by Krikor Jabourian Nakhleh Nehmeh Yara YounesDocument33 pagesHypertension: by Krikor Jabourian Nakhleh Nehmeh Yara YounesHamza DibNo ratings yet
- Pharmacological-Management-of-HypertensionDocument35 pagesPharmacological-Management-of-Hypertensiontf.almutairi88No ratings yet
- Cardiac Glycosides - ScribdDocument12 pagesCardiac Glycosides - ScribdmiznahNo ratings yet
- Drugs Used in HF IIDocument40 pagesDrugs Used in HF IIJamal LudinNo ratings yet
- Summary of Product Characteristics 1 Name of The Medicinal ProductDocument9 pagesSummary of Product Characteristics 1 Name of The Medicinal Productddandan_2No ratings yet
- Cardiovascular Agents Group 1 Parmacology ReportingDocument415 pagesCardiovascular Agents Group 1 Parmacology ReportingMajestic RavenNo ratings yet
- Hypertension Lecture3: Pharmacological TreatmentDocument25 pagesHypertension Lecture3: Pharmacological TreatmentRam NiwasNo ratings yet
- Hypertension: Silent KillerDocument28 pagesHypertension: Silent KilleribratiNo ratings yet
- Cardiovascular PharmacotherapyDocument32 pagesCardiovascular PharmacotherapyFarahEzzlynnNo ratings yet
- Anti-Anginal Drugs ExplainedDocument19 pagesAnti-Anginal Drugs ExplainedAnusha ZubairNo ratings yet
- Acute Decompensated Heart FailureDocument31 pagesAcute Decompensated Heart Failure568563No ratings yet
- Management of Heart Failure: OutlineDocument27 pagesManagement of Heart Failure: OutlineBoetik AlifiaNo ratings yet
- Heart Disease Drugs: Cardiac Glycosides, Antihypertensives & DiureticsDocument24 pagesHeart Disease Drugs: Cardiac Glycosides, Antihypertensives & Diureticsblah4020No ratings yet
- Cardiotonic Drugs for Heart FailureDocument42 pagesCardiotonic Drugs for Heart FailureHannaNo ratings yet
- Cardio DrugsDocument68 pagesCardio DrugsIconMaicoNo ratings yet
- Heart Failure and Antidysrhythmic DrugsDocument38 pagesHeart Failure and Antidysrhythmic DrugsYza Belle RamoNo ratings yet
- Review of Advancements in Heart Failure 81220Document65 pagesReview of Advancements in Heart Failure 81220Dr MustafaNo ratings yet
- Aritmia Dan Kardiotonik Eng UciDocument36 pagesAritmia Dan Kardiotonik Eng UciUci RamadhantyNo ratings yet
- AntiHypertensives (Autosaved)Document64 pagesAntiHypertensives (Autosaved)UsamaNo ratings yet
- Antihypertensive Drugs RTDocument41 pagesAntihypertensive Drugs RTMaherNo ratings yet
- Session 24 Heart FailureDocument15 pagesSession 24 Heart Failuredreampurpose97No ratings yet
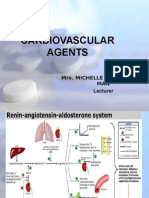
- Cardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerDocument131 pagesCardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerNiala AlmarioNo ratings yet
- Heat Failure DrugsDocument8 pagesHeat Failure DrugsDaniel MwiluNo ratings yet
- Anti HypertensionDocument63 pagesAnti HypertensionAngga CahyadiNo ratings yet
- HypertensionDocument54 pagesHypertensionBadri KarkiNo ratings yet
- Anoosha Roll#21Document19 pagesAnoosha Roll#21Anusha ZubairNo ratings yet
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Principles of Pharmacokinetics (PKDocument25 pagesPrinciples of Pharmacokinetics (PKSimonNo ratings yet
- Adrenergic Drugs: ''Sympathomimetics & Sympatholytics"Document17 pagesAdrenergic Drugs: ''Sympathomimetics & Sympatholytics"SimonNo ratings yet
- EpilepsyDocument10 pagesEpilepsySimonNo ratings yet
- Principles of Pharmacokinetics (PKDocument25 pagesPrinciples of Pharmacokinetics (PKSimonNo ratings yet
- 01 - Introduction To PharmacologyDocument9 pages01 - Introduction To PharmacologySimonNo ratings yet
- Drug StudyDocument3 pagesDrug StudyNica NiñoNo ratings yet
- Kode Icd XDocument8 pagesKode Icd Xraniasyahcandra67% (6)
- 2001 FRACP Written Examination Paediatrics & ChildDocument48 pages2001 FRACP Written Examination Paediatrics & ChildMedicEdNo ratings yet
- Price List PT BMP: Nama Obat Satuan Stok Harga Nett++ (RP)Document98 pagesPrice List PT BMP: Nama Obat Satuan Stok Harga Nett++ (RP)apriantiNo ratings yet
- T 1234029783 11845985 Nursing Crib Com Nursing Care Plan Dengue FeverDocument2 pagesT 1234029783 11845985 Nursing Crib Com Nursing Care Plan Dengue Feversamantha cortezNo ratings yet
- G 3333333@356Document46 pagesG 3333333@356abrar aliNo ratings yet
- Orchitis 160406115741Document28 pagesOrchitis 160406115741alyne100% (1)
- Peritonitis PDFDocument1 pagePeritonitis PDFHoney MacabuhayNo ratings yet
- Im Boards Rationalized ExamDocument21 pagesIm Boards Rationalized Examesbat07No ratings yet
- List Item Stock Opname SyrupDocument8 pagesList Item Stock Opname Syrupahmad zainyNo ratings yet
- Liver Abscess Clinical Presentation - History, Physical Examination, ComplicationsDocument2 pagesLiver Abscess Clinical Presentation - History, Physical Examination, ComplicationsAdi Kurnia100% (1)
- Median Rhomboid GlossitisDocument2 pagesMedian Rhomboid Glossitisdianzalerti9240No ratings yet
- BPS Oncology Pharmacy Practice ExamDocument11 pagesBPS Oncology Pharmacy Practice Examiman100% (3)
- Isi FornasDocument239 pagesIsi FornasVrizskiNo ratings yet
- Chapter 31 Thyroid and Antithyroid DrugsDocument37 pagesChapter 31 Thyroid and Antithyroid Drugsjrflores1284No ratings yet
- Update Stok 19 Maret 2019Document14 pagesUpdate Stok 19 Maret 2019ayu RachmawatiNo ratings yet
- CPG Dengue Signs Admission Risk FactorsDocument3 pagesCPG Dengue Signs Admission Risk FactorsKristine Jade OdtujanNo ratings yet
- Cell Wall Synthesis InhibitorsDocument57 pagesCell Wall Synthesis InhibitorsNica MendozaNo ratings yet
- Medcomei2013 PDFDocument238 pagesMedcomei2013 PDFVanesa PaniaguaNo ratings yet
- OSCE DermaDocument8 pagesOSCE DermaameerabestNo ratings yet
- Mupirocin Drug StudyDocument1 pageMupirocin Drug StudyArthur Christopher Corpuz0% (1)
- Acute Rheumatic FeverDocument50 pagesAcute Rheumatic Feversunaryo lNo ratings yet
- Jurnal Febris (Demam) 3Document8 pagesJurnal Febris (Demam) 3Maymunah 07No ratings yet
- HYDROCELEDocument12 pagesHYDROCELEChristin Feliana SitanggangNo ratings yet
- Supplements: Otc Prescription CosmeticsDocument18 pagesSupplements: Otc Prescription CosmeticsMaria Angela Del GallegoNo ratings yet
- What Is ImpetigoDocument4 pagesWhat Is ImpetigoKate Mylhen Espenido EnerlanNo ratings yet
- Drug Summary Table: Chapter 37 Pharmacology of Cancer: Genome Synthesis, Stability, and MaintenanceDocument6 pagesDrug Summary Table: Chapter 37 Pharmacology of Cancer: Genome Synthesis, Stability, and MaintenanceRita GameiroNo ratings yet
- Alphex PDFDocument1 pageAlphex PDFIdalia OrtegaNo ratings yet
- Obat Anestesi Intravena: Obat Untuk Dosis OOA DOADocument1 pageObat Anestesi Intravena: Obat Untuk Dosis OOA DOAdede rianiNo ratings yet
- GBS Case StudyDocument2 pagesGBS Case Studyjperry107No ratings yet