You might also like
- A Cancer Companion: An Oncologist's Advice on Diagnosis, Treatment, and RecoveryFrom EverandA Cancer Companion: An Oncologist's Advice on Diagnosis, Treatment, and RecoveryNo ratings yet
- Predictive Values, Sensitivity and Specificity in Clinical VirologyDocument26 pagesPredictive Values, Sensitivity and Specificity in Clinical Virologymichele garciaNo ratings yet
- Screening of DiseasesDocument50 pagesScreening of Diseasesravi_rohilla100% (1)
- 29 Sep 2023principles and Predictive Value of ScreeningDocument29 pages29 Sep 2023principles and Predictive Value of Screening1.barron.whiteNo ratings yet
- Screening: Department of Public Health Medical School, University of PécsDocument38 pagesScreening: Department of Public Health Medical School, University of PécsESSA GHAZWANI100% (1)
- Summary of Diagnostic Test Accuracy For BR PDFDocument33 pagesSummary of Diagnostic Test Accuracy For BR PDFOlfat ashrafNo ratings yet
- Epi Lec 5Document40 pagesEpi Lec 5Dr. Mahbub Alam MahfuzNo ratings yet
- Chapter 8Document26 pagesChapter 8Nathnael GebNo ratings yet
- 3 ScreeningDocument33 pages3 ScreeningIbrahim Ahmed OsmanNo ratings yet
- Screening TestDocument31 pagesScreening Testd3mooz13No ratings yet
- Critical Appraisal Cross Sectional Case ControlDocument76 pagesCritical Appraisal Cross Sectional Case ControlAndita SyabanaNo ratings yet
- Chemical Pathology Workshop II - Diagnostic Theory in Chemical Pathology (2017.11.14)Document57 pagesChemical Pathology Workshop II - Diagnostic Theory in Chemical Pathology (2017.11.14)Arthur Chang100% (1)
- Screening Tests by BastaDocument14 pagesScreening Tests by BastaKanar MahmoodNo ratings yet
- Screening Tests: Accuracy, Validity and CriteriaDocument28 pagesScreening Tests: Accuracy, Validity and CriteriaruthNo ratings yet
- Diagnostic Studies PEBHC Workshop December 2015Document77 pagesDiagnostic Studies PEBHC Workshop December 2015Nursyamsi AhmadNo ratings yet
- Evidence-Based Medicine: StatisticsDocument42 pagesEvidence-Based Medicine: StatisticsAHMED .KNo ratings yet
- Screening CriteriaDocument40 pagesScreening CriteriaDhrubajyoti Sen100% (1)
- Diagnostic Studies Annette PluddemannDocument58 pagesDiagnostic Studies Annette Pluddemanne.K.e.kNo ratings yet
- Screening TestsDocument35 pagesScreening Testsapi-3699330No ratings yet
- Screening 2010Document29 pagesScreening 2010seethahereNo ratings yet
- Chapter 8 ScreeningDocument29 pagesChapter 8 ScreeningEstiv W. StigNo ratings yet
- ScreeningDocument41 pagesScreeningReham M NagatyNo ratings yet
- Epi L 13Document39 pagesEpi L 13abo ageelNo ratings yet
- Concept of ScreeningDocument39 pagesConcept of ScreeningKanika SatijaNo ratings yet
- Description of Performance of TestDocument72 pagesDescription of Performance of TestSurendra AwasthiNo ratings yet
- Epi-Lessons 5Document44 pagesEpi-Lessons 5Najeeb haiderNo ratings yet
- Probabilities in Clinical Medicine: Mohammad Saifur Rohman, Md. PHDDocument41 pagesProbabilities in Clinical Medicine: Mohammad Saifur Rohman, Md. PHDerlisaNo ratings yet
- Ix. Screening in Disease ControlDocument42 pagesIx. Screening in Disease ControlyohanesNo ratings yet
- Screening - Master - 2022Document57 pagesScreening - Master - 2022Kanwal KhanNo ratings yet
- Interpretation of Diagnostic Screening TestsDocument33 pagesInterpretation of Diagnostic Screening TestsAMELIA CAROLINA HERRERA BRICEÑONo ratings yet
- 4 - Clinical EpidemiologyDocument8 pages4 - Clinical EpidemiologyDiana Mitrea100% (1)
- Screening Test Sensitivity vs SpecificityDocument7 pagesScreening Test Sensitivity vs SpecificityKinuPatel100% (2)
- Diagnosis: Highlights: Cita Rosita Sigit PrakoeswaDocument68 pagesDiagnosis: Highlights: Cita Rosita Sigit PrakoeswaAdniana NareswariNo ratings yet
- Screening Tests: Sensitivity, Specificity, PPV and NPVDocument35 pagesScreening Tests: Sensitivity, Specificity, PPV and NPVpaperpin27100% (1)
- Interpreting Diagnostic Tests: Ian Mcdowell Department of Epidemiology & Community Medicine January 2010Document30 pagesInterpreting Diagnostic Tests: Ian Mcdowell Department of Epidemiology & Community Medicine January 2010AntenehNo ratings yet
- Screening in Public HealthDocument35 pagesScreening in Public HealthOkeleke EbukaNo ratings yet
- BiostastisticsDocument21 pagesBiostastisticsRiin ĐặngNo ratings yet
- ScreeningDocument24 pagesScreeningM7MD SHOWNo ratings yet
- Epi & StatisticsDocument135 pagesEpi & StatisticsFatma AlSayeghNo ratings yet
- Sensitivity Vs SpecificityDocument16 pagesSensitivity Vs SpecificitydwataNo ratings yet
- Sensitivity and SpecificityDocument18 pagesSensitivity and SpecificityIris BallajNo ratings yet
- 5 ScreeningDocument50 pages5 ScreeningmariamNo ratings yet
- Epidemiology - Lecture 4Document81 pagesEpidemiology - Lecture 4Samuel Betobaye DjikoinguéNo ratings yet
- Screening TestDocument22 pagesScreening TestRabea DiaNo ratings yet
- PHPS30020 Clinical Epidemiology Prof Fitzpatrick 2023 PostedDocument38 pagesPHPS30020 Clinical Epidemiology Prof Fitzpatrick 2023 PostedKatie NolanNo ratings yet
- Disease ScreeningDocument41 pagesDisease ScreeningFreelance LeagueNo ratings yet
- SKRENINGDocument40 pagesSKRENINGPuti NoviandiniNo ratings yet
- Conditional Probability and Medical TestsDocument20 pagesConditional Probability and Medical TestsRuslan MalovanyyNo ratings yet
- Screening: To Sort Out Apparently Well Persons Who Probably Have A Disease From Those Who Probably Do Not."Document24 pagesScreening: To Sort Out Apparently Well Persons Who Probably Have A Disease From Those Who Probably Do Not."Munir AkhtarNo ratings yet
- Diagnosis Dan Skrining: I.Riwanto F.K. UNDIP Semarang Mata Kuliah Epidemiologi Lanjut S3. I. Kedokteran UNDIPDocument40 pagesDiagnosis Dan Skrining: I.Riwanto F.K. UNDIP Semarang Mata Kuliah Epidemiologi Lanjut S3. I. Kedokteran UNDIPRetno SucianaNo ratings yet
- Diagnostic Testing-1Document45 pagesDiagnostic Testing-1Ali HassanNo ratings yet
- Screening_dr Heba MahmoudDocument45 pagesScreening_dr Heba MahmoudMerna IbrahimNo ratings yet
- ScreeningDocument55 pagesScreeningephremtigabie7No ratings yet
- Assessing The Validity and Reliability of Diagnostic and Screening TestsDocument38 pagesAssessing The Validity and Reliability of Diagnostic and Screening Testssarguss1467% (3)
- Evidence-Based Diagnosis in Physical TherapyDocument32 pagesEvidence-Based Diagnosis in Physical TherapyHari25885No ratings yet
- Evaluation of Diagnostic and Screening Tests: Validity and ReliabilityDocument27 pagesEvaluation of Diagnostic and Screening Tests: Validity and Reliabilitykoyilada jhahnavi100% (1)
- Critical Appraisal Checklist For An Article On Diagnosis or ScreeningDocument4 pagesCritical Appraisal Checklist For An Article On Diagnosis or ScreeningAnonymous dOrzIvlNo ratings yet
- Seren Award Masterclass 2Document13 pagesSeren Award Masterclass 2Angelika LauNo ratings yet
- MM20802 NotesDocument15 pagesMM20802 NotesdanishNo ratings yet
- Anticancer Effects of Constituents of Herbs Targeting OsteosarcomaDocument8 pagesAnticancer Effects of Constituents of Herbs Targeting OsteosarcomaOstazNo ratings yet
- JCM 11 00699Document20 pagesJCM 11 00699OstazNo ratings yet
- Progress of Biomaterials For BoneDocument11 pagesProgress of Biomaterials For BoneOstazNo ratings yet
- Potential Anticancer PropertiesDocument28 pagesPotential Anticancer PropertiesOstazNo ratings yet
- Potential of Natural Products in Osteosarcoma TreatmentDocument21 pagesPotential of Natural Products in Osteosarcoma TreatmentOstazNo ratings yet
- Resveratrol in Management of Bone and Spinal CancersDocument12 pagesResveratrol in Management of Bone and Spinal CancersOstazNo ratings yet
- Function of P2 Receptors in Primary Bone CancerDocument20 pagesFunction of P2 Receptors in Primary Bone CancerOstazNo ratings yet
- Skaven ChangelogDocument1 pageSkaven ChangelogOstazNo ratings yet
- Opinion Piece: Patient-Specific Implants May Be The Next Big Thing in Spinal SurgeryDocument11 pagesOpinion Piece: Patient-Specific Implants May Be The Next Big Thing in Spinal SurgeryOstazNo ratings yet
- CARE Checklist English 2013 PDFDocument1 pageCARE Checklist English 2013 PDFNithin NairNo ratings yet
- MainDocument10 pagesMainOstazNo ratings yet
- Sutures Versus Staples For Skin Closure in Orthopaedic Surgery: Meta-AnalysisDocument9 pagesSutures Versus Staples For Skin Closure in Orthopaedic Surgery: Meta-AnalysisOstazNo ratings yet
- Fifty Years of Bone TumorsDocument7 pagesFifty Years of Bone TumorsOstazNo ratings yet
- Warhammer ChangelogDocument8 pagesWarhammer ChangelogOstazNo ratings yet
- Sicotj 3 16Document10 pagesSicotj 3 16OstazNo ratings yet
- MainDocument8 pagesMainOstazNo ratings yet
- How To Identify and Share Your ValuesDocument3 pagesHow To Identify and Share Your ValuesOstazNo ratings yet
- Implications of 3-Dimensional Printed Spinal Implants On The Outcomes in Spine SurgeryDocument10 pagesImplications of 3-Dimensional Printed Spinal Implants On The Outcomes in Spine SurgeryOstazNo ratings yet
- HHS Public Access: 3D Printing of Highly Stretchable and Tough Hydrogels Into Complex, Cellularized StructuresDocument13 pagesHHS Public Access: 3D Printing of Highly Stretchable and Tough Hydrogels Into Complex, Cellularized StructuresOstazNo ratings yet
- JRM-CC: Clinical CommunicationsDocument7 pagesJRM-CC: Clinical CommunicationsOstazNo ratings yet
- Wang 2020Document14 pagesWang 2020OstazNo ratings yet
- 3d-Printed Patient-Specific Applications in Orthopedics: Orthopedic Research and Reviews DoveDocument10 pages3d-Printed Patient-Specific Applications in Orthopedics: Orthopedic Research and Reviews DoveOstazNo ratings yet
- MainDocument9 pagesMainOstazNo ratings yet
- Conventional Vs 3-Dimensional Printed Cast Wear ComfortDocument5 pagesConventional Vs 3-Dimensional Printed Cast Wear ComfortOstazNo ratings yet
- 10.1177 0300060520924250Document12 pages10.1177 0300060520924250OstazNo ratings yet
- Bmri2021 5018791Document15 pagesBmri2021 5018791OstazNo ratings yet
- Accepted Manuscript: 10.1016/j.ijsu.2018.07.012Document39 pagesAccepted Manuscript: 10.1016/j.ijsu.2018.07.012OstazNo ratings yet
- Perspectives of 3D Printing Technology in Orthopaedic SurgeryDocument7 pagesPerspectives of 3D Printing Technology in Orthopaedic SurgeryOstaz100% (1)
- 10.1177 0300060520924250Document12 pages10.1177 0300060520924250OstazNo ratings yet
- Bmri2021 5018791Document15 pagesBmri2021 5018791OstazNo ratings yet
- MICROORGANISMS Class 8Document2 pagesMICROORGANISMS Class 8AyushNo ratings yet
- Case StudyDocument2 pagesCase StudyClaire MachicaNo ratings yet
- CBCR Joint Pain Student VersionDocument4 pagesCBCR Joint Pain Student VersionNika GianashviliNo ratings yet
- © 2017 Lanternfish ESL @Document5 pages© 2017 Lanternfish ESL @DanniNo ratings yet
- Tiket Juragan GombalDocument3 pagesTiket Juragan Gombaldhebys suryaniNo ratings yet
- Rhenock, Sikkim Village ReportDocument101 pagesRhenock, Sikkim Village Reportankitsaxena88No ratings yet
- VGG16 Based Knee Osteoarthritis Grading Using X-Ray ImagesDocument8 pagesVGG16 Based Knee Osteoarthritis Grading Using X-Ray ImagesIJRASETPublicationsNo ratings yet
- REVISI (Adelita Setiawan 2)Document7 pagesREVISI (Adelita Setiawan 2)Adelita SetiawanNo ratings yet
- MolnupiravirDocument7 pagesMolnupiravirConcepStore PyNo ratings yet
- Surgical Hand Hygiene PosterDocument2 pagesSurgical Hand Hygiene PosterIrenne WibowoNo ratings yet
- Biochemistry Papers MSUDocument20 pagesBiochemistry Papers MSUShiv BhattNo ratings yet
- In Class Assignment Module 10193 11 SanieDocument3 pagesIn Class Assignment Module 10193 11 SanieXyruz Redulfin100% (5)
- 1119 P1 Cefr Reading ModuleDocument181 pages1119 P1 Cefr Reading ModuleLueiNo ratings yet
- Epistaksis Pada Polip Nasal: September 2022Document10 pagesEpistaksis Pada Polip Nasal: September 2022FitrianiNo ratings yet
- Focused Ultrasonography For Septic Shock ResuscitationDocument7 pagesFocused Ultrasonography For Septic Shock ResuscitationntnquynhproNo ratings yet
- How Do We Walk?: Sujay Galen PT PHD FheaDocument52 pagesHow Do We Walk?: Sujay Galen PT PHD FheaColleen JohnsonNo ratings yet
- Gender-Dysphoric-Incongruene Persons, Guidelines JCEM 2017Document35 pagesGender-Dysphoric-Incongruene Persons, Guidelines JCEM 2017Manel EMNo ratings yet
- Magsaysay Memorial College of Zambales, IncDocument4 pagesMagsaysay Memorial College of Zambales, IncJoanne CuestaNo ratings yet
- The Dental Plaque Biofilm MatrixDocument25 pagesThe Dental Plaque Biofilm MatrixTasha FarahNo ratings yet
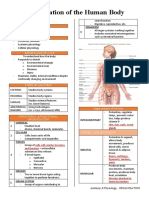
- Organization of the Human BodyDocument8 pagesOrganization of the Human BodyAly HannahNo ratings yet
- J American Geriatrics Society - 2023 - American Geriatrics Society 2023 Updated AGS Beers Criteria For PotentiallyDocument30 pagesJ American Geriatrics Society - 2023 - American Geriatrics Society 2023 Updated AGS Beers Criteria For PotentiallyMikeNo ratings yet
- SHAHMEERDocument29 pagesSHAHMEERMosa AbdullahNo ratings yet
- 3.5 PHARMA ANTI MYCOBACTERIAL AGENTSpdfDocument18 pages3.5 PHARMA ANTI MYCOBACTERIAL AGENTSpdfJanet SantosNo ratings yet
- YAWNEY, C. Ways of Seeing IllnessDocument8 pagesYAWNEY, C. Ways of Seeing IllnessfernandoNo ratings yet
- DefibrillationDocument4 pagesDefibrillationNeha BhardwajNo ratings yet
- Acr-Nasci-Sir-Spr Practice Parameter For The Performance and Interpretation of Body Computed Tomography Angiography (Cta)Document15 pagesAcr-Nasci-Sir-Spr Practice Parameter For The Performance and Interpretation of Body Computed Tomography Angiography (Cta)kirim mammoNo ratings yet
- Urinary SystemDocument9 pagesUrinary SystemMary Joyce RamosNo ratings yet
- MCQs Breast Pathology 1Document5 pagesMCQs Breast Pathology 1Ishita SinghNo ratings yet
- TRAUMATIC BRAIN INJURY MEDICAL SURGICAL NURSINGDocument48 pagesTRAUMATIC BRAIN INJURY MEDICAL SURGICAL NURSINGErica Keil MoleNo ratings yet
- The Effect of Smoking OnDocument42 pagesThe Effect of Smoking OnAndreina AcevedoNo ratings yet