You might also like
- Managments in Oncology 13OCTDocument49 pagesManagments in Oncology 13OCTM ANo ratings yet
- Radiation TherapyDocument4 pagesRadiation Therapypanniyin selvanNo ratings yet
- Non Surgical Treatment Modalities of SCCHN: Presentation by Post Gradute StudentDocument113 pagesNon Surgical Treatment Modalities of SCCHN: Presentation by Post Gradute StudentZubair VajaNo ratings yet
- Recent Advances in Radiation Oncology: DR M Spoorthi Shelometh Department of Radiation OncologyDocument53 pagesRecent Advances in Radiation Oncology: DR M Spoorthi Shelometh Department of Radiation Oncologyspoorthi shelomethNo ratings yet
- Radiation TherapyDocument7 pagesRadiation TherapyMeenakshi VyasNo ratings yet
- Linac Report FINALDocument32 pagesLinac Report FINALJasmine KaurNo ratings yet
- Radiation TherapyDocument58 pagesRadiation TherapyRichard Allan SolivenNo ratings yet
- SMRT Radiation Therapy IntroDocument18 pagesSMRT Radiation Therapy IntroDar WebNo ratings yet
- Assignment On Radiation TherapyDocument16 pagesAssignment On Radiation TherapyAxsa AlexNo ratings yet
- Radiation Therapy 2013Document59 pagesRadiation Therapy 2013AydinNo ratings yet
- Radiation Therapy OverviewDocument5 pagesRadiation Therapy OverviewMae CeaesarNo ratings yet
- Radiation TherapyDocument11 pagesRadiation Therapyrnnr2159No ratings yet
- Oncology Nursing Care Cancer Treatment ModalitiesDocument90 pagesOncology Nursing Care Cancer Treatment ModalitiesMaviel Maratas SarsabaNo ratings yet
- Ways Radiation Is Used in Medicine - Cobalt 60 Radiotherapy MachineDocument22 pagesWays Radiation Is Used in Medicine - Cobalt 60 Radiotherapy MachineKavidu KeshanNo ratings yet
- Radiation TherapyDocument28 pagesRadiation Therapypalakkhurana012No ratings yet
- AccesfobDocument19 pagesAccesfobCristinaNo ratings yet
- Cancer Therapy Modalities & Side EffectsDocument9 pagesCancer Therapy Modalities & Side EffectsNeweeJoonYowNo ratings yet
- Radiotherapy For CancerDocument12 pagesRadiotherapy For CancerAshfiya ShaikhNo ratings yet
- Principles of Radiotherapy 2016Document85 pagesPrinciples of Radiotherapy 2016Ali B. SafadiNo ratings yet
- Tumour and Their MXDocument39 pagesTumour and Their MXadNo ratings yet
- Use of Radiation in Diagnosis and TherapeuticsDocument7 pagesUse of Radiation in Diagnosis and TherapeuticsADITYAROOP PATHAKNo ratings yet
- Andrew Idoko Radiology GROUP 332 1. The Concept of Radical and Palliative Treatment. Indications, Contraindications Dose Limits. ExamplesDocument5 pagesAndrew Idoko Radiology GROUP 332 1. The Concept of Radical and Palliative Treatment. Indications, Contraindications Dose Limits. ExamplesdreNo ratings yet
- Principles of chemotherapy and radiotherapy for gynaecological cancersDocument7 pagesPrinciples of chemotherapy and radiotherapy for gynaecological cancersNora100% (3)
- Clinical Practice 4: RadiotherapyDocument46 pagesClinical Practice 4: RadiotherapyallordNo ratings yet
- Clinical Practice 4: RadiotherapyDocument27 pagesClinical Practice 4: RadiotherapyallordNo ratings yet
- Clinical Practice 4: Radiotherapy Lecture 5 & 6Document28 pagesClinical Practice 4: Radiotherapy Lecture 5 & 6allordNo ratings yet
- Principles of RadiotherapyDocument41 pagesPrinciples of Radiotherapywabaly100% (1)
- Nursing ManagementDocument19 pagesNursing ManagementAbby Trisha MadularaNo ratings yet
- (RADIO 250) LEC 10 Radiation OncologyDocument3 pages(RADIO 250) LEC 10 Radiation OncologyWilliam PinzonNo ratings yet
- Radiation TherapyDocument13 pagesRadiation TherapyJils SureshNo ratings yet
- Principles of Radiation OncologyDocument22 pagesPrinciples of Radiation OncologyGina RNo ratings yet
- Radiation Therapy: Group 4 and 5Document29 pagesRadiation Therapy: Group 4 and 5Anonymous 596wAK78eCNo ratings yet
- OverviewDocument6 pagesOverviewarakbaeNo ratings yet
- Shahan Mumraiz Khan-2017 076Document48 pagesShahan Mumraiz Khan-2017 076zaminazzNo ratings yet
- Management of Patient With CancerDocument52 pagesManagement of Patient With CancerAru VermaNo ratings yet
- Title - BT Treatment Procedure For Vaginal CarcinomaDocument21 pagesTitle - BT Treatment Procedure For Vaginal CarcinomaparvezNo ratings yet
- RT For General PublicDocument24 pagesRT For General Publicraheel252100% (1)
- Radiation Therapy For CancerDocument65 pagesRadiation Therapy For CancermelNo ratings yet
- RadiotherapyDocument60 pagesRadiotherapyAARYANo ratings yet
- Article 56252 PDFDocument9 pagesArticle 56252 PDFandre halimNo ratings yet
- RT 307Document153 pagesRT 307Lyht TVNo ratings yet
- Radiography Safety ProcedureDocument9 pagesRadiography Safety ProcedureأحمدآلزهوNo ratings yet
- Head and Neck Cancer - Head and Neck Cancer Treatment - Treatment of Head and Neck in India: Omegahospitals, HyderabadDocument2 pagesHead and Neck Cancer - Head and Neck Cancer Treatment - Treatment of Head and Neck in India: Omegahospitals, HyderabadRyan ThompsonNo ratings yet
- Update of Radiotherapy For Skin Cancer: Review ArticlesDocument8 pagesUpdate of Radiotherapy For Skin Cancer: Review ArticlesOscar Frizzi100% (1)
- Radiation Therapy for Cancer TreatmentDocument9 pagesRadiation Therapy for Cancer TreatmentKartik SharmaNo ratings yet
- Radiation Therapy: Surgery Ward WorkDocument9 pagesRadiation Therapy: Surgery Ward WorkKartik SharmaNo ratings yet
- RADIOTHERAPHYDocument20 pagesRADIOTHERAPHYMuhammad Hafiz KarimNo ratings yet
- Use of Radioactive in MedicalDocument28 pagesUse of Radioactive in MedicalroseyacobNo ratings yet
- What is Interventional Radiology in 38 CharactersDocument8 pagesWhat is Interventional Radiology in 38 CharactersNIMKY EMBER B. CLAMOHOYNo ratings yet
- Understanding Radiation TherapyDocument24 pagesUnderstanding Radiation Therapyabhilashreddy45No ratings yet
- Quiz 2024Document10 pagesQuiz 2024bijay kumarNo ratings yet
- CANCER TREATMENT OPTIONSDocument28 pagesCANCER TREATMENT OPTIONSAbirami SankarNo ratings yet
- Principles of Oncology SurgeryDocument40 pagesPrinciples of Oncology SurgeryMaimoona AimanNo ratings yet
- Stereotactic RadiosurgeryDocument38 pagesStereotactic RadiosurgeryHussein mmNo ratings yet
- Brachytherapy Procedures and ApplicationsDocument5 pagesBrachytherapy Procedures and ApplicationsChiara Tenorio ÜNo ratings yet
- Radiation Oncology Fractionation SchedulesDocument31 pagesRadiation Oncology Fractionation Schedulesoncology KMC-KnlNo ratings yet
- Non Operative MX of TumorsDocument108 pagesNon Operative MX of TumorsRamjas ChoudharyNo ratings yet
- RT For Healthcare ProfessionalsDocument35 pagesRT For Healthcare Professionalsvamsi NathNo ratings yet
- Cancer Textbook 4 (Cancer Treatment and Ovarian Cancer)From EverandCancer Textbook 4 (Cancer Treatment and Ovarian Cancer)No ratings yet
- Radiotherapy of Liver CancerFrom EverandRadiotherapy of Liver CancerJinsil SeongNo ratings yet
- Diseases of Oral Cavity: - Dr. Amar KumarDocument61 pagesDiseases of Oral Cavity: - Dr. Amar KumarSudhanshu ShekharNo ratings yet
- HerniaDocument26 pagesHerniaSudhanshu ShekharNo ratings yet
- Tracheostomy Procedure GuideDocument18 pagesTracheostomy Procedure GuideSudhanshu ShekharNo ratings yet
- The Vermiform AppendixDocument17 pagesThe Vermiform AppendixSudhanshu ShekharNo ratings yet
- FNHA First Nations Health Benefits Mental Health Provider ListDocument17 pagesFNHA First Nations Health Benefits Mental Health Provider ListJoel PanganibanNo ratings yet
- Competition Commission of India Economics Study Material Amp NotesDocument3 pagesCompetition Commission of India Economics Study Material Amp NotesRaghav DhillonNo ratings yet
- Fetal Mummification in CowsDocument22 pagesFetal Mummification in CowsTahseen AlamNo ratings yet
- Public Service Commission, West Bengal: Notice Inviting Expression of Interest For Enlistment As LawyersDocument3 pagesPublic Service Commission, West Bengal: Notice Inviting Expression of Interest For Enlistment As LawyersITI JobNo ratings yet
- Hieu Doan: The Path of PowerDocument206 pagesHieu Doan: The Path of Powerhulu12100% (1)
- Emergency Mang TraumaDocument16 pagesEmergency Mang Traumaeliemaalouf4No ratings yet
- List of Islamic Schools in Toronto To Apply For JobsDocument5 pagesList of Islamic Schools in Toronto To Apply For JobsgetsaifurNo ratings yet
- DFA vs NLRC Immunity DisputeDocument7 pagesDFA vs NLRC Immunity DisputeThrees SeeNo ratings yet
- Campus Hiring Presentation - PART 1Document35 pagesCampus Hiring Presentation - PART 1Zalak ShahNo ratings yet
- Calculus For EngineersDocument268 pagesCalculus For EngineersSr_Tabosa100% (1)
- Lecture 2 2014 Random Errors in Chemical AnalysisDocument24 pagesLecture 2 2014 Random Errors in Chemical AnalysisRobert EdwardsNo ratings yet
- Tawassulan Fik TjakrabuanaDocument6 pagesTawassulan Fik TjakrabuanafikditasresNo ratings yet
- 5 All India Mobile Database SampleDocument15 pages5 All India Mobile Database Sampleali khan Saifi100% (1)
- Holistic Retreat, Doi Saket, Chiang MaiDocument4 pagesHolistic Retreat, Doi Saket, Chiang MaiShireenNo ratings yet
- FORM B1 Photocopiables 3CDocument2 pagesFORM B1 Photocopiables 3CAnka SchoolNo ratings yet
- LM1 Toc 25141Document1 pageLM1 Toc 25141Sotiris AthinaiosNo ratings yet
- Complete Dermatology NotesDocument41 pagesComplete Dermatology NotesSetlhare MotsamaiNo ratings yet
- Retaining Wall With PilesDocument7 pagesRetaining Wall With PilesEngineering KaizenNo ratings yet
- Dokumen - Tips - Ielts and Toefl Made Easy George John Efc and Is The First Coherence PDFDocument2 pagesDokumen - Tips - Ielts and Toefl Made Easy George John Efc and Is The First Coherence PDFPayal SethiNo ratings yet
- Leopoldo Jeremias Vs Estate of MarianoDocument1 pageLeopoldo Jeremias Vs Estate of MarianoGee LorinNo ratings yet
- Canon Sus 2016 e 03Document2 pagesCanon Sus 2016 e 03Roxanne Tacy SantiagoNo ratings yet
- Phase Diagram of Three-Component Liquid SystemDocument11 pagesPhase Diagram of Three-Component Liquid SystemVanessa Denise Aguilar100% (2)
- Tle Fos 9 11 q1 WK 7 d1Document6 pagesTle Fos 9 11 q1 WK 7 d1REYMOND SUMAYLONo ratings yet
- Selection of Hazard Evaluation Techniques PDFDocument16 pagesSelection of Hazard Evaluation Techniques PDFdediodedNo ratings yet
- LF ReportDocument32 pagesLF ReportKrisLarrNo ratings yet
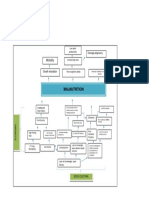
- Problem Tree Analysis MalnutritionDocument1 pageProblem Tree Analysis MalnutritionMho Dsb50% (6)
- Health Teaching Plan - AttitudeDocument2 pagesHealth Teaching Plan - AttitudeFaller TrixieNo ratings yet
- Selling & Negotiation SkillsDocument70 pagesSelling & Negotiation SkillsMojo JOjoNo ratings yet
- The Snouters - Form and Life of - Harald StumpkeDocument126 pagesThe Snouters - Form and Life of - Harald StumpkeAlberto Humanes MuñozNo ratings yet
- Techniques in Neuroanatomical ResearchDocument404 pagesTechniques in Neuroanatomical ResearchVlad TomaNo ratings yet