You might also like
- Retinal Diseases 230210 210855Document108 pagesRetinal Diseases 230210 210855RgdNo ratings yet
- Retinal Detachment and HomoeopathyDocument7 pagesRetinal Detachment and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Retinal DetachmentDocument8 pagesRetinal DetachmentJohanLazuardiNo ratings yet
- Retinal DetachmentDocument3 pagesRetinal DetachmentzeejayNo ratings yet
- 1retinal DetachmentDocument5 pages1retinal Detachmentsunny_jr_No ratings yet
- Retinal DetachmentDocument31 pagesRetinal DetachmentEko KunaryagiNo ratings yet
- Retinal DetachmentDocument3 pagesRetinal DetachmentRownald Lakandula PanuncialNo ratings yet
- Retinal DetachmentDocument14 pagesRetinal DetachmentChikita Artia Sari100% (1)
- Retinal DetachmentDocument14 pagesRetinal DetachmentPui_Yee_Siow_6303No ratings yet
- Cataract PPT FinalDocument37 pagesCataract PPT FinalSibi John90% (21)
- Retinaldetachmentnew WORSDocument51 pagesRetinaldetachmentnew WORSMuthulakshmiNo ratings yet
- Vitreous Gel Eye Retinal Detachment OphthalmologistDocument12 pagesVitreous Gel Eye Retinal Detachment OphthalmologistLesTrechSaNo ratings yet
- Ablasio RetinaDocument6 pagesAblasio RetinaDan DanisaNo ratings yet
- Retinal Detachments and The Current Trends of TreatmentDocument10 pagesRetinal Detachments and The Current Trends of Treatmentapi-235387260No ratings yet
- Corneal Dystrophies: Retinal DetachmentDocument6 pagesCorneal Dystrophies: Retinal DetachmentMarissa AsimNo ratings yet
- Mata Tenang Visus Turun MendadakDocument74 pagesMata Tenang Visus Turun MendadakYeni AnggrainiNo ratings yet
- Pemicu 1 PENGINDRAAN C2Document113 pagesPemicu 1 PENGINDRAAN C2CcNo ratings yet
- Retinal Detachment Is A Disorder of The Eye in Which The Retina Peels Away From Its Underlying Layer of Support TissueDocument5 pagesRetinal Detachment Is A Disorder of The Eye in Which The Retina Peels Away From Its Underlying Layer of Support TissuejobinbionicNo ratings yet
- Retinal Detachment Nava Joanna D.Document10 pagesRetinal Detachment Nava Joanna D.JoanneNBondocNo ratings yet
- Indikasi Operasi KatarakDocument3 pagesIndikasi Operasi KatarakAsdiana NurNo ratings yet
- Cataract: Antony Halim I4061162030Document50 pagesCataract: Antony Halim I4061162030Gilang PramanayudhaNo ratings yet
- Cataract ReportDocument59 pagesCataract ReportRuDy RaviNo ratings yet
- Corneal Dystrophies: Retinal DetachmentDocument5 pagesCorneal Dystrophies: Retinal DetachmentCake ManNo ratings yet
- Retinal DetachmentDocument32 pagesRetinal Detachmentc/risaaq yuusuf ColoowNo ratings yet
- Ophthalmology: Anatomy of The LensDocument35 pagesOphthalmology: Anatomy of The Lensمحمد عبدالوهاب ابراهيم الطباطبائيNo ratings yet
- Dada 2007Document4 pagesDada 2007asfwegereNo ratings yet
- Retinal DetachmentDocument21 pagesRetinal DetachmentRose O'SullivanNo ratings yet
- Pemicu 1 Pengindraan c2Document113 pagesPemicu 1 Pengindraan c2CcNo ratings yet
- Concept MapDocument4 pagesConcept MapCasison Mark ArrysonNo ratings yet
- Surgical Management of MyopiaDocument23 pagesSurgical Management of MyopiaMohamed Ghanem100% (4)
- Advances in The Treatment of Rhegmatogenous Retinal DetachmentDocument8 pagesAdvances in The Treatment of Rhegmatogenous Retinal DetachmentFathirNo ratings yet
- Retinaldetachment 170518024801Document47 pagesRetinaldetachment 170518024801GetLyricsNo ratings yet
- Terminology: Nuclear Sclerotic CataractsDocument4 pagesTerminology: Nuclear Sclerotic CataractsBenjamin NgNo ratings yet
- 2014FeltgenDABenglish PDFDocument14 pages2014FeltgenDABenglish PDFNurul ArdaniNo ratings yet
- 2014FeltgenDABenglish PDFDocument14 pages2014FeltgenDABenglish PDFNurul ArdaniNo ratings yet
- CataractDocument24 pagesCataractNeela Kandan100% (1)
- Retinal DetachmentDocument6 pagesRetinal DetachmentNader Smadi100% (3)
- Course 7 I, IIDocument17 pagesCourse 7 I, IItaliya. shvetzNo ratings yet
- CataractDocument45 pagesCataractAmit Martin100% (2)
- Diskusi Topik - Ali Mustagi - Mata Normal Visus Turun PerlahanDocument73 pagesDiskusi Topik - Ali Mustagi - Mata Normal Visus Turun PerlahanalimustagialgiNo ratings yet
- Emergency Management: Retinal DetachmentDocument1 pageEmergency Management: Retinal DetachmentSitti HazrinaNo ratings yet
- AAO Reading VitrectomyDocument65 pagesAAO Reading VitrectomydestiNo ratings yet
- Management of CataractDocument25 pagesManagement of Cataractapi-3742497No ratings yet
- Retinal Detachment: Practice EssentialsDocument6 pagesRetinal Detachment: Practice EssentialsDeasy Arindi PutriNo ratings yet
- CATARACTDocument25 pagesCATARACTDea NabilaNo ratings yet
- Introduction, Health History, GordonsDocument10 pagesIntroduction, Health History, GordonsKayelyn-Rose CombateNo ratings yet
- Cataract CasestudyDocument3 pagesCataract CasestudyJamal AgontongNo ratings yet
- Lens by DR - Haider AswadDocument7 pagesLens by DR - Haider AswadcwkmrqkhjjNo ratings yet
- Eye Disorders: Presented by Carmelita Ramos, RNDocument65 pagesEye Disorders: Presented by Carmelita Ramos, RNJayme_Galang_7078100% (1)
- Retinal Physician - Visualization in Vitrectomy - An UpdateDocument12 pagesRetinal Physician - Visualization in Vitrectomy - An UpdateDr. M. Hannan JamilNo ratings yet
- What Is The Treatment For Retinal Detachment?: CryotherapyDocument2 pagesWhat Is The Treatment For Retinal Detachment?: Cryotherapyanbarasan2006No ratings yet
- Bosch ErDocument8 pagesBosch ErPhilip McNelsonNo ratings yet
- Retinal DetachmentDocument21 pagesRetinal Detachmentณัช เกษมNo ratings yet
- Retinal DetachmentDocument16 pagesRetinal DetachmentCandice Lim Swee LingNo ratings yet
- What Is The Meaning of FloatersDocument2 pagesWhat Is The Meaning of FloatersdrtheeyeNo ratings yet
- Retinal Detachment: Case Report Operating RoomDocument30 pagesRetinal Detachment: Case Report Operating RoomCarlo Joseph Intal LlacerNo ratings yet
- Ophthalmology - Diseases of VitreousDocument5 pagesOphthalmology - Diseases of VitreousjbtcmdtjjvNo ratings yet
- Cataract: Sarah Jane B. Aca-Ac BSN-3 Page 1770-1773Document13 pagesCataract: Sarah Jane B. Aca-Ac BSN-3 Page 1770-1773De Sesto Rhys CarloNo ratings yet
- Low Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsFrom EverandLow Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsNo ratings yet
- Clinical Ophthalmology for UndergraduatesFrom EverandClinical Ophthalmology for UndergraduatesRating: 4 out of 5 stars4/5 (5)
- Bio-Assay Test On The Result of Indoor Residual Spraying (IRS) Application in Malaria Disease ControlDocument6 pagesBio-Assay Test On The Result of Indoor Residual Spraying (IRS) Application in Malaria Disease ControlVivi YolandhaNo ratings yet
- CopasDocument65 pagesCopasTomyNo ratings yet
- SJS FixDocument11 pagesSJS FixVivi YolandhaNo ratings yet
- SJS FixDocument11 pagesSJS FixVivi YolandhaNo ratings yet
- Thorax Abdomen ExaminationDocument39 pagesThorax Abdomen Examinationmelanita_99No ratings yet
- International Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikDocument56 pagesInternational Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikpriyagerardNo ratings yet
- Too Tired EDS and Fatigue - Brad TinkleDocument34 pagesToo Tired EDS and Fatigue - Brad TinkleGèniaNo ratings yet
- Fnac of Thyroid - 102717Document13 pagesFnac of Thyroid - 102717Lal RuattlingaNo ratings yet
- Investigations For PneumoniaDocument27 pagesInvestigations For PneumoniaRoshana Mallawaarachchi0% (1)
- Anthroposophical Approach To Cancer Rita Leroi MDDocument26 pagesAnthroposophical Approach To Cancer Rita Leroi MD144bob144No ratings yet
- Medical Self Declaration FormDocument1 pageMedical Self Declaration FormVarun SinglaNo ratings yet
- Articulo 4Document8 pagesArticulo 4Sonia GarcíaNo ratings yet
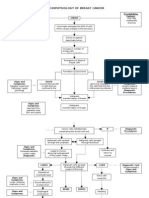
- Pathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsDocument3 pagesPathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsKevin Ercia100% (1)
- Surgery Shelf Review - 2Document34 pagesSurgery Shelf Review - 2Coral Srinivasa Ramalu75% (4)
- Intestinal ObstructionDocument59 pagesIntestinal ObstructionGeorge GuruNo ratings yet
- What Is ParaplegiaDocument3 pagesWhat Is Paraplegiaalok_kumar_guptaNo ratings yet
- Drug Bulletin: Antipsychotic MonitoringDocument4 pagesDrug Bulletin: Antipsychotic MonitoringMuhammad NaufalNo ratings yet
- Nosocomial InfectionDocument57 pagesNosocomial InfectionFaith Ho100% (1)
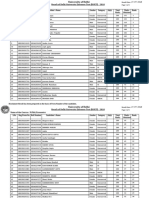
- Name of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Document5 pagesName of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Saiganesh RameshNo ratings yet
- Testing For Tuberculosis (TB) : Tuberculin Skin Test (TST)Document2 pagesTesting For Tuberculosis (TB) : Tuberculin Skin Test (TST)Aluh L DiniNo ratings yet
- Infections Dr. Mowafy 2nd EditionDocument26 pagesInfections Dr. Mowafy 2nd EditionMohammed RisqNo ratings yet
- Test TitleDocument3 pagesTest TitleMarkNo ratings yet
- USPSTF A and B RecomendationsDocument5 pagesUSPSTF A and B RecomendationsVishala MishraNo ratings yet
- Proceedings of The 16th Italian Association of Equine Veterinarians CongressDocument4 pagesProceedings of The 16th Italian Association of Equine Veterinarians CongressCabinet VeterinarNo ratings yet
- Urnal Vox Sanguinis - 2023 - Pons - Prevalence of Red Blood Cell Alloantibodies Among Blood Donors in The French Military BloodDocument5 pagesUrnal Vox Sanguinis - 2023 - Pons - Prevalence of Red Blood Cell Alloantibodies Among Blood Donors in The French Military BloodFauzan.ANo ratings yet
- "Bloody Scours": Swine DysenteryDocument29 pages"Bloody Scours": Swine DysenteryleaNo ratings yet
- Electrical System of The HeartDocument4 pagesElectrical System of The HeartEldhaNo ratings yet
- Cues/ Data Cues/ Data: Family Nursing Problem Family Nursing ProblemDocument14 pagesCues/ Data Cues/ Data: Family Nursing Problem Family Nursing ProblemAriane Rose Saria CedronNo ratings yet
- DAFTAR PUSTAKA Referat Ca MammaeDocument5 pagesDAFTAR PUSTAKA Referat Ca MammaeAulia JanerNo ratings yet
- HCIA Study Guide 2023Document22 pagesHCIA Study Guide 2023consultasluisfloresdrNo ratings yet
- Normal ObDocument31 pagesNormal ObShai EstrellerNo ratings yet
- Sentence Outline Africa HypertensionggeneDocument2 pagesSentence Outline Africa HypertensionggeneYzel Senining100% (3)
- 1 s2.0 S014067362300020X MainDocument14 pages1 s2.0 S014067362300020X MainGERIATRIA 72No ratings yet
- Leg English PDFDocument1 pageLeg English PDFBracelethNicole E. NicolasNo ratings yet