You might also like
- Pemicu 1 Pengindraan c2Document113 pagesPemicu 1 Pengindraan c2CcNo ratings yet
- Chronic Visual LossDocument7 pagesChronic Visual LossJim Jose AntonyNo ratings yet
- Special Sense EYEDocument74 pagesSpecial Sense EYEprekshya shresthaNo ratings yet
- Function RpeDocument4 pagesFunction RpeKristine Ramos100% (1)
- Ophthalmology: Anatomy of The LensDocument35 pagesOphthalmology: Anatomy of The Lensمحمد عبدالوهاب ابراهيم الطباطبائيNo ratings yet
- Retinal AnatomyDocument86 pagesRetinal AnatomySean ScogginsNo ratings yet
- Course 7 I, IIDocument17 pagesCourse 7 I, IItaliya. shvetzNo ratings yet
- Cornea Structure and Keratoconus IntroductionDocument33 pagesCornea Structure and Keratoconus IntroductionMuhammad MustafaNo ratings yet
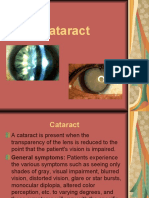
- Cataract PPT FinalDocument37 pagesCataract PPT FinalSibi John90% (20)
- Cet 5Document4 pagesCet 5jumi26No ratings yet
- Senile Cataract (Age-Related Cataract) : Practice Essentials, Background, PathophysiologyDocument6 pagesSenile Cataract (Age-Related Cataract) : Practice Essentials, Background, PathophysiologyadliahghaisaniNo ratings yet
- Senile Cataract (Age-Related Cataract) - Practice Essentials, Background, PathophysiologyDocument5 pagesSenile Cataract (Age-Related Cataract) - Practice Essentials, Background, PathophysiologyAhmad FahroziNo ratings yet
- Cataract ReportDocument59 pagesCataract ReportRuDy RaviNo ratings yet
- Paper MataDocument18 pagesPaper Matairawaty purbaNo ratings yet
- Final TouchDocument49 pagesFinal TouchmalathiNo ratings yet
- CataractDocument63 pagesCataractMutti KakarNo ratings yet
- Assessment of The EyeDocument4 pagesAssessment of The EyeAira Nicole ROMASNo ratings yet
- UntitledDocument45 pagesUntitledc/risaaq yuusuf ColoowNo ratings yet
- Abnormalities of EyeDocument74 pagesAbnormalities of EyeHikmat UllahNo ratings yet
- Michael G. Glasspool FRCS, DO (Auth.) - Atlas of Ophthalmology-Springer Netherlands (1982) PDFDocument117 pagesMichael G. Glasspool FRCS, DO (Auth.) - Atlas of Ophthalmology-Springer Netherlands (1982) PDFInna BujorNo ratings yet
- Eyes and Vision PresentationDocument142 pagesEyes and Vision Presentationrhimineecat71100% (1)
- The EyeDocument48 pagesThe Eyezyrine jhen100% (1)
- Cataract: Sarah Jane B. Aca-Ac BSN-3 Page 1770-1773Document13 pagesCataract: Sarah Jane B. Aca-Ac BSN-3 Page 1770-1773De Sesto Rhys CarloNo ratings yet
- BY: Achin Pant 3 Year MbbsDocument59 pagesBY: Achin Pant 3 Year MbbsMitali MohanNo ratings yet
- GlaucomaDocument18 pagesGlaucomaOncología CdsNo ratings yet
- Senile Cataract: DR SyedDocument28 pagesSenile Cataract: DR SyedShahzada KhanNo ratings yet
- PSSS-Mata Tenang Visus Turun PerlahanDocument48 pagesPSSS-Mata Tenang Visus Turun PerlahanYesi 'faiqa Putir100% (1)
- Ocular USG of Post EyeDocument14 pagesOcular USG of Post EyeAL MARIA MEDNo ratings yet
- Retinal Diseases 230210 210855Document108 pagesRetinal Diseases 230210 210855RgdNo ratings yet
- Proiect Nerv OpticDocument7 pagesProiect Nerv Opticiuliabucur92No ratings yet
- The Physics of Light and Color - Human Vision and Color Perception - Olympus LSDocument14 pagesThe Physics of Light and Color - Human Vision and Color Perception - Olympus LSmarialopezmartinez424No ratings yet
- Cataract NotesDocument4 pagesCataract NotesJeremy LauNo ratings yet
- Bo 402 (32301721022)Document8 pagesBo 402 (32301721022)AvinabaNo ratings yet
- Terjemahan Vaughan DDocument20 pagesTerjemahan Vaughan DMelina Indah Sari100% (1)
- ANATO - Campos VisuaisDocument11 pagesANATO - Campos VisuaishelbertpalmieroNo ratings yet
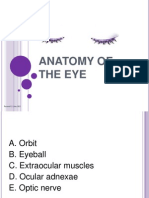
- ANATOMY & PHYSIOLOGY OF THE EYEDocument70 pagesANATOMY & PHYSIOLOGY OF THE EYEArif MohammadNo ratings yet
- Histology of The EyeDocument91 pagesHistology of The EyeFazira EkmaNo ratings yet
- Introduction To Ophthalmology: by DR - Bakhtiar Q. JafDocument41 pagesIntroduction To Ophthalmology: by DR - Bakhtiar Q. JafChristian JaraNo ratings yet
- Yoga & Eye - Anatomy and PhysiologyDocument73 pagesYoga & Eye - Anatomy and Physiologysachi sharma0% (1)
- MyopiaDocument11 pagesMyopiablueiceNo ratings yet
- Vitreoretina: DR - Reinne Natali Christine, SPM Dept. Ilmu Penyakit Mata FK Uki / Rsu FK UkiDocument45 pagesVitreoretina: DR - Reinne Natali Christine, SPM Dept. Ilmu Penyakit Mata FK Uki / Rsu FK UkitusuksedotanNo ratings yet
- Сataract 09Document32 pagesСataract 09somebody_maNo ratings yet
- Retinal Detachment: Causes, Symptoms and Treatment Options Under 40 CharactersDocument32 pagesRetinal Detachment: Causes, Symptoms and Treatment Options Under 40 Charactersc/risaaq yuusuf ColoowNo ratings yet
- Far Eastern University - Posterior Segment Evaluation TechniquesDocument13 pagesFar Eastern University - Posterior Segment Evaluation TechniquesCzara DyNo ratings yet
- Ophthalmology for Oxford and Duke-Elder examsDocument4 pagesOphthalmology for Oxford and Duke-Elder examsBenjamin NgNo ratings yet
- Lens and CataractDocument31 pagesLens and CataractReinhard TuerahNo ratings yet
- Glossary of termsDocument6 pagesGlossary of termsAlberto Ybañez CastañedaNo ratings yet
- Presentation (1) - 1Document13 pagesPresentation (1) - 1Uzair AkhterNo ratings yet
- Cataract: Antony Halim I4061162030Document50 pagesCataract: Antony Halim I4061162030Gilang PramanayudhaNo ratings yet
- 7 Lens and Cataract 1Document57 pages7 Lens and Cataract 1Devi Melissa RiupassaNo ratings yet
- Glaucoma FinalDocument40 pagesGlaucoma FinalAdoma SportsNo ratings yet
- Optic Atrophy :major Review March 2010, Kerala Journal of Ophthalmology, Devendra V. Venkatramani Et AlDocument6 pagesOptic Atrophy :major Review March 2010, Kerala Journal of Ophthalmology, Devendra V. Venkatramani Et AlNavojit ChowdhuryNo ratings yet
- Topic Presentation CataractDocument11 pagesTopic Presentation Cataractjyoti singhNo ratings yet
- Eye Disorders: Presented by Carmelita Ramos, RNDocument65 pagesEye Disorders: Presented by Carmelita Ramos, RNJayme_Galang_7078100% (1)
- 4-Lens and CataractDocument59 pages4-Lens and CataractSa'adah Munawaroh HDNo ratings yet
- WPR 2Document5 pagesWPR 2ishika mohanNo ratings yet
- Eye and AdnexaDocument22 pagesEye and AdnexaWadabiNo ratings yet
- Low Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsFrom EverandLow Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsNo ratings yet
- Conjuntivitis SMDocument9 pagesConjuntivitis SMIntan N HNo ratings yet
- Refer atDocument2 pagesRefer atCcNo ratings yet
- Ocular Chemical Injuries and Their Management PDFDocument4 pagesOcular Chemical Injuries and Their Management PDFCcNo ratings yet
- KGD P6 Emergency Medicine: TambahanDocument127 pagesKGD P6 Emergency Medicine: TambahanCcNo ratings yet
- Synopsis of Causation: Dermatitis (Eczema) Including Occupational DermatitisDocument19 pagesSynopsis of Causation: Dermatitis (Eczema) Including Occupational DermatitisCcNo ratings yet
- Gizi Hun KweDocument1 pageGizi Hun KweCcNo ratings yet
- Pembahasan Pemicu 1Document56 pagesPembahasan Pemicu 1CcNo ratings yet
- Grand Escape: (Weathering With You)Document3 pagesGrand Escape: (Weathering With You)CcNo ratings yet
- KGD P6 Emergency Medicine: TambahanDocument127 pagesKGD P6 Emergency Medicine: TambahanCcNo ratings yet
- Grand EscapeDocument3 pagesGrand EscapeCcNo ratings yet
- Pemicu 4 Saraf C2Document111 pagesPemicu 4 Saraf C2CcNo ratings yet
- Jurnal DMDocument19 pagesJurnal DMCcNo ratings yet
- Whole-Grain and Blood Lipid PDFDocument17 pagesWhole-Grain and Blood Lipid PDFCcNo ratings yet
- Fluid ManagementDocument6 pagesFluid ManagementCcNo ratings yet
- Kasus UROLOGIDocument6 pagesKasus UROLOGICcNo ratings yet
- Kasus UROLOGIDocument56 pagesKasus UROLOGICcNo ratings yet
- Problem 6 Pleno 2Document149 pagesProblem 6 Pleno 2CcNo ratings yet
- Kasus UROLOGIDocument56 pagesKasus UROLOGICcNo ratings yet
- Pemicu 1 Blok UrogenitalDocument173 pagesPemicu 1 Blok UrogenitalCcNo ratings yet
- 10 6th ProblemDocument112 pages10 6th ProblemCcNo ratings yet
- Acute GastroenteritisDocument28 pagesAcute GastroenteritisSiergs Smith GervacioNo ratings yet
- Intake AssessmentDocument2 pagesIntake Assessmentyourzxtruly0% (1)
- Amit BiomedSignalDocument14 pagesAmit BiomedSignalDr-Amit Kumar SinghNo ratings yet
- Clinical Aspects of PneumothoraxDocument3 pagesClinical Aspects of PneumothoraxelisabethNo ratings yet
- Dermtimes - Vitiligo Treatment SuccessDocument2 pagesDermtimes - Vitiligo Treatment SuccessradqudahNo ratings yet
- Gender and Society Module 2Document12 pagesGender and Society Module 2Mary Rose Distura OnceNo ratings yet
- AneurysmDocument10 pagesAneurysmMarquel CulmerNo ratings yet
- The Facts About Mental Illness in The ElderlyDocument7 pagesThe Facts About Mental Illness in The Elderlyastha singhNo ratings yet
- 29 - Toronto Notes 2011 - Urology PDFDocument44 pages29 - Toronto Notes 2011 - Urology PDFDewa Gede Reza Sanjaya0% (1)
- Cardiac Surgery in The Adult-3rd EditionDocument1,729 pagesCardiac Surgery in The Adult-3rd EditionFlorentina Negoita96% (26)
- Complications Bariatric SurgeryDocument8 pagesComplications Bariatric SurgeryThita Orrego100% (1)
- Program Book11Document1,124 pagesProgram Book11heocon857351No ratings yet
- Caduet (Dr. Ismahun Maret 2009)Document41 pagesCaduet (Dr. Ismahun Maret 2009)Yulia SumarnaNo ratings yet
- Interaksi Obat Obat MaagDocument8 pagesInteraksi Obat Obat MaagSiti NurohmahhNo ratings yet
- Fogsi ChecklistDocument131 pagesFogsi ChecklistParimi VinodNo ratings yet
- Ethicon Wound Closure ManualDocument126 pagesEthicon Wound Closure Manualkeish193100% (3)
- Tumors of The Jaw and Oral MucosaDocument18 pagesTumors of The Jaw and Oral MucosaDaniela LeonteNo ratings yet
- Jordanian Surgical Society - PPT LastDocument166 pagesJordanian Surgical Society - PPT LastNessreen Jamal100% (1)
- HAI Surveillance ChallengesDocument78 pagesHAI Surveillance ChallengesMichael EdmondNo ratings yet
- Effect of Intraoperative Dexmedetomidine On Post-Craniotomy PainDocument9 pagesEffect of Intraoperative Dexmedetomidine On Post-Craniotomy PainIva SantikaNo ratings yet
- Pharmacology NotesDocument6 pagesPharmacology NotesHarsh PawarNo ratings yet
- Ppha Immunizing Pharmacists Certification ProgramDocument27 pagesPpha Immunizing Pharmacists Certification ProgramRoberto ChaileNo ratings yet
- Drug Discovery and Development Lecture NotesDocument75 pagesDrug Discovery and Development Lecture NotesJameel BakhshNo ratings yet
- Reference RangesDocument8 pagesReference RangesKru PrimeNo ratings yet
- Vaishya 2014Document26 pagesVaishya 2014quyhienminhNo ratings yet
- Residual Breast Tissue After Mastectomy, How Often and Where It Is LocatedDocument11 pagesResidual Breast Tissue After Mastectomy, How Often and Where It Is LocatedBunga Tri AmandaNo ratings yet
- Pharma Medical Director Cardiology in NYC Resume Ronald HabermanDocument3 pagesPharma Medical Director Cardiology in NYC Resume Ronald HabermanRonaldHabermanNo ratings yet
- Echelon Revision Casestudies 71380632Document16 pagesEchelon Revision Casestudies 71380632Dipen ShahNo ratings yet
- Homoeopathic Drug Pictures PDFDocument718 pagesHomoeopathic Drug Pictures PDFNimesh PatelNo ratings yet
- Ergonomics in CarpentryDocument32 pagesErgonomics in CarpentrypsyishNo ratings yet