You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
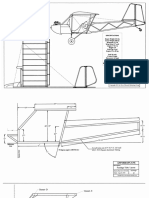
- Plans PDFDocument49 pagesPlans PDFEstevam Gomes de Azevedo85% (34)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- From Input To Affordance: Social-Interactive Learning From An Ecological Perspective Leo Van Lier Monterey Institute Oflntemational StudiesDocument15 pagesFrom Input To Affordance: Social-Interactive Learning From An Ecological Perspective Leo Van Lier Monterey Institute Oflntemational StudiesKayra MoslemNo ratings yet
- The Acceptability of Rubber Tree Sap (A As An Alternative Roof SealantDocument7 pagesThe Acceptability of Rubber Tree Sap (A As An Alternative Roof SealantHannilyn Caldeo100% (2)
- Clinical Competency ChecklistDocument9 pagesClinical Competency ChecklistSHAFIQNo ratings yet
- University of Health Sciences Lahore: Postgraduate Entrance Test 2020Document1 pageUniversity of Health Sciences Lahore: Postgraduate Entrance Test 2020SHAFIQNo ratings yet
- Log Sheet 2Document4 pagesLog Sheet 2SHAFIQNo ratings yet
- Log Sheet 4Document4 pagesLog Sheet 4SHAFIQNo ratings yet
- Log Sheet 3Document4 pagesLog Sheet 3SHAFIQNo ratings yet
- Log Sheet 1Document4 pagesLog Sheet 1SHAFIQNo ratings yet
- Orthopedic SOAPDocument3 pagesOrthopedic SOAPSHAFIQNo ratings yet
- Antenatal Care: Presented byDocument36 pagesAntenatal Care: Presented bySHAFIQNo ratings yet
- Ubaid Khan KmuDocument11 pagesUbaid Khan KmuSHAFIQNo ratings yet
- ENT Clinic SOAP NotesDocument3 pagesENT Clinic SOAP NotesSHAFIQNo ratings yet
- Fluids & Electrolytes Imbalance KMUDocument37 pagesFluids & Electrolytes Imbalance KMUSHAFIQNo ratings yet
- Unit IV Power & Politics in NursingDocument18 pagesUnit IV Power & Politics in NursingSHAFIQNo ratings yet
- KMU Blood DisorderDocument43 pagesKMU Blood DisorderSHAFIQNo ratings yet
- Kmu Therapeutic Play & CommunicationDocument26 pagesKmu Therapeutic Play & CommunicationSHAFIQNo ratings yet
- Pediatric Health Nursing Unit I BSN Year III, Semester V: by Hidayatullah Khan BSN, DPN & MSN Kmu-InsDocument59 pagesPediatric Health Nursing Unit I BSN Year III, Semester V: by Hidayatullah Khan BSN, DPN & MSN Kmu-InsSHAFIQNo ratings yet
- Care of Child With Head InjuryDocument34 pagesCare of Child With Head InjurySHAFIQNo ratings yet
- Assessment of Neoborn FinalDocument91 pagesAssessment of Neoborn FinalSHAFIQNo ratings yet
- Unit II Pathophysiology of CVS: by Hidayat Khan KMUDocument17 pagesUnit II Pathophysiology of CVS: by Hidayat Khan KMUSHAFIQNo ratings yet
- Musculoskeletal Disorders KMUDocument18 pagesMusculoskeletal Disorders KMUSHAFIQNo ratings yet
- Environmental Health: by Mr. Imran Yousafzai BSN (Pak), MSPH (Pak), PGHRHM (UK), MHPE (Pak)Document43 pagesEnvironmental Health: by Mr. Imran Yousafzai BSN (Pak), MSPH (Pak), PGHRHM (UK), MHPE (Pak)SHAFIQNo ratings yet
- Sorah Fatiha TarjumaDocument1 pageSorah Fatiha TarjumaSHAFIQNo ratings yet
- Unit II Management Functions: by Group: 2 Sana Saleem Abrar Tariq Jamil Institute of Nursing Sciences, KMUDocument45 pagesUnit II Management Functions: by Group: 2 Sana Saleem Abrar Tariq Jamil Institute of Nursing Sciences, KMUSHAFIQNo ratings yet
- Haider Ali CHN PaperDocument9 pagesHaider Ali CHN PaperSHAFIQ0% (2)
- Health Management Information SystemDocument7 pagesHealth Management Information SystemSHAFIQNo ratings yet
- Demography/Global Health & Health TransitionDocument22 pagesDemography/Global Health & Health TransitionSHAFIQNo ratings yet
- Community Health Nurseing Unit1Document34 pagesCommunity Health Nurseing Unit1SHAFIQ100% (1)
- Assad Ullah TahirDocument10 pagesAssad Ullah TahirSHAFIQNo ratings yet
- Fariha HameedDocument6 pagesFariha HameedSHAFIQNo ratings yet
- Shamasa KiranDocument9 pagesShamasa KiranSHAFIQNo ratings yet
- HashmatDocument9 pagesHashmatSHAFIQNo ratings yet
- Tuberculosis PowerpointDocument69 pagesTuberculosis PowerpointCeline Villo100% (1)
- HCPL 316J 000eDocument34 pagesHCPL 316J 000eElyes MbarekNo ratings yet
- Nissan Copper LTDDocument11 pagesNissan Copper LTDankit_shahNo ratings yet
- Arduino Oscilloscope ProjectDocument12 pagesArduino Oscilloscope ProjectSathya Narayan100% (1)
- 5G Transport Slice Control in End-To-End 5G NetworksDocument19 pages5G Transport Slice Control in End-To-End 5G NetworksmorganNo ratings yet
- Rail Vehicle DynamicsDocument55 pagesRail Vehicle DynamicsdfNo ratings yet
- Indor Lighting DesignDocument33 pagesIndor Lighting DesignRajesh MalikNo ratings yet
- Electric ScootorDocument40 pagesElectric Scootor01fe19bme079No ratings yet
- FRP Handrail Fittings CatalogDocument6 pagesFRP Handrail Fittings CatalogAl Adel MorenoNo ratings yet
- Murata High Voltage CeramicDocument38 pagesMurata High Voltage CeramictycristinaNo ratings yet
- Catalogo Aesculap PDFDocument16 pagesCatalogo Aesculap PDFHansNo ratings yet
- Implicit Explicit SignalsDocument8 pagesImplicit Explicit SignalsVersoza Nel100% (2)
- Stepan Formulation 926Document2 pagesStepan Formulation 926Moaz SiddigNo ratings yet
- Tree Growth CharacteristicsDocument9 pagesTree Growth CharacteristicsMunganNo ratings yet
- 41z S4hana2021 Set-Up en XXDocument46 pages41z S4hana2021 Set-Up en XXHussain MulthazimNo ratings yet
- LET General Math ReviewerDocument7 pagesLET General Math ReviewerMarco Rhonel Eusebio100% (1)
- Soldier of Fortune PDFDocument208 pagesSoldier of Fortune PDFNixel SpielNo ratings yet
- Purpose in LifeDocument1 pagePurpose in Lifeaashish95100% (1)
- SAT Practice TestDocument77 pagesSAT Practice TestfhfsfplNo ratings yet
- Nivel VV-VW Board User Guide enDocument5 pagesNivel VV-VW Board User Guide enHarveyWishtartNo ratings yet
- Updated G10 Class Routine Effective From 12 January 2023Document1 pageUpdated G10 Class Routine Effective From 12 January 2023NiloyNo ratings yet
- Straight LineDocument15 pagesStraight LineAyanNo ratings yet
- AssessmentDocument3 pagesAssessmentpalflaxNo ratings yet
- Save Water SpeechDocument4 pagesSave Water SpeechHari Prakash Shukla0% (1)
- D 6000Document6 pagesD 6000os_ja@hotmail.comNo ratings yet
- Bomba MixerDocument2 pagesBomba MixerBinelli79No ratings yet
- Cost Analysis - Giberson Art GlassDocument3 pagesCost Analysis - Giberson Art GlassSessy Saly50% (2)