You might also like
- Nasio - 1Document38 pagesNasio - 1VusiNo ratings yet
- PharmacoeconomicsDocument54 pagesPharmacoeconomicsAsfa MarediaNo ratings yet
- Health Economic MethodsDocument14 pagesHealth Economic MethodsVerónica Garavito SanabriaNo ratings yet
- Principles of PharmacoeconomicsDocument9 pagesPrinciples of Pharmacoeconomicsshafinaz12No ratings yet
- Define Economic Evaluation With An Appropriate Diagram. DefinitionDocument8 pagesDefine Economic Evaluation With An Appropriate Diagram. DefinitionrojinaNo ratings yet
- Economics Evaluation: Faculty of Public Health, University of Muhammadiyah Jakarta Ridhwan Fauzi, MPH 08121914211Document31 pagesEconomics Evaluation: Faculty of Public Health, University of Muhammadiyah Jakarta Ridhwan Fauzi, MPH 08121914211synyster92xNo ratings yet
- Introduction To Pharmacoeconomics: Almut G. Winterstein, PH.DDocument43 pagesIntroduction To Pharmacoeconomics: Almut G. Winterstein, PH.DjunifitrahNo ratings yet
- Economic Evaluations of Clinical Pharmacy Services 2001–2005Document59 pagesEconomic Evaluations of Clinical Pharmacy Services 2001–2005Indra PratamaNo ratings yet
- Dwi Endarti-Penetapan Prioritas Masalah Kajian FE 21 Sept 22Document26 pagesDwi Endarti-Penetapan Prioritas Masalah Kajian FE 21 Sept 22zaiNo ratings yet
- Parmacoecnomics 2Document43 pagesParmacoecnomics 2Aina ButtNo ratings yet
- CBA - s17 - Class NotesDocument78 pagesCBA - s17 - Class NotesEric YoungNo ratings yet
- Far Mako Eko NomiDocument59 pagesFar Mako Eko NomiLina LinuxNo ratings yet
- Basic Economic AnalysisDocument19 pagesBasic Economic AnalysisTUSHAR MANDALENo ratings yet
- Session 8 Cost Analysis (Compatibility Mode)Document25 pagesSession 8 Cost Analysis (Compatibility Mode)Behar AbdurahemanNo ratings yet
- Basic of PharmacoeconomicsDocument34 pagesBasic of Pharmacoeconomicssridwiwulan dariNo ratings yet
- Chapter 14Document38 pagesChapter 14Screw Soft (Screw Soft Channel)No ratings yet
- Economic Evaluation in Health CareDocument18 pagesEconomic Evaluation in Health CareYogesh ChandraNo ratings yet
- Types of Economic Evaluation in Healthcare 1Document26 pagesTypes of Economic Evaluation in Healthcare 1Ozkar ZaldivarNo ratings yet
- Session 3 BUSI 863 PostDocument28 pagesSession 3 BUSI 863 PostKelann BelfonNo ratings yet
- 4 - Outcome AssessmentDocument88 pages4 - Outcome Assessmentgunanti1307No ratings yet
- Pharmacoeconomics: Pharmacoeconomics Has Been Defined As The Description and The Analysis of The Cost of Drug TherapyDocument6 pagesPharmacoeconomics: Pharmacoeconomics Has Been Defined As The Description and The Analysis of The Cost of Drug TherapySreya SanilNo ratings yet
- 3.13.08 - COI Cost MinimizationDocument16 pages3.13.08 - COI Cost Minimizationapi-3723612No ratings yet
- EconomicsDocument12 pagesEconomicsk289rmzzb6No ratings yet
- Pengantar Evaluasi EkonomiDocument29 pagesPengantar Evaluasi EkonomiyumnaNo ratings yet
- Cost Benefit Analysis (CBA) & Cost Effectivenes Analysis (CEA)Document17 pagesCost Benefit Analysis (CBA) & Cost Effectivenes Analysis (CEA)Maher GamingNo ratings yet
- Intro To Health EconomicsDocument34 pagesIntro To Health EconomicsRasha ElzenyNo ratings yet
- Pharmacoeconomics Lecture OneDocument10 pagesPharmacoeconomics Lecture OneMohammed al-dairiNo ratings yet
- CCA Template WebsiteDocument11 pagesCCA Template WebsiteSumitAggarwalNo ratings yet
- Chapter 3Document21 pagesChapter 3ShubhashriNo ratings yet
- Cost-Effectiveness of Asthmazolimide for AsthmaDocument20 pagesCost-Effectiveness of Asthmazolimide for AsthmaEric YoungNo ratings yet
- CAP Lecture 4Document32 pagesCAP Lecture 4reissitamu1No ratings yet
- Pharmacoeconomics - : Lebanese International University School of Pharmacy Fall 2021-2022Document18 pagesPharmacoeconomics - : Lebanese International University School of Pharmacy Fall 2021-2022undeadrebornNo ratings yet
- Analisis Efektivitas-Biaya: Prih SarniantoDocument18 pagesAnalisis Efektivitas-Biaya: Prih SarniantoM YogaNo ratings yet
- Cost EffectivenessDocument22 pagesCost EffectivenessEdalyn CapiliNo ratings yet
- Priority Setting - Economics in Health CareDocument23 pagesPriority Setting - Economics in Health CarePeni M. SaptoargoNo ratings yet
- Engaging the C-Suite to Advance Pharmacy PracticeDocument47 pagesEngaging the C-Suite to Advance Pharmacy Practiceibson045001256No ratings yet
- Evaluating Health Programs' Economic ImpactDocument19 pagesEvaluating Health Programs' Economic ImpactRatih Ayunani IrawanNo ratings yet
- Ch2 Measuring and Estimating CostsDocument20 pagesCh2 Measuring and Estimating CostsAhmad MakhloufNo ratings yet
- Introduction of pharmacoeconomic ﻲﻟﻮﻟا ﺪﺒﻋ /دDocument18 pagesIntroduction of pharmacoeconomic ﻲﻟﻮﻟا ﺪﺒﻋ /دMaido TeNo ratings yet
- SROI in Public HealthDocument14 pagesSROI in Public Healthyuda00No ratings yet
- Lecture 8 - CBA AnalysisDocument35 pagesLecture 8 - CBA AnalysisVũ QuânNo ratings yet
- PHAP AssignmentDocument9 pagesPHAP Assignmentarmand bayoranNo ratings yet
- Health Economic Evaluation: From Theory To Practice: Assoc Prof DR Arthorn RiewpaiboonDocument34 pagesHealth Economic Evaluation: From Theory To Practice: Assoc Prof DR Arthorn RiewpaiboonTiti SulistiowatiNo ratings yet
- Methods of Pharmacoeconomic AnalysisDocument19 pagesMethods of Pharmacoeconomic AnalysisDoaa BadarnehNo ratings yet
- PharmacoeconomicsDocument21 pagesPharmacoeconomicsAina Butt100% (1)
- Health economics in 40 charactersDocument4 pagesHealth economics in 40 charactersleprof ahmedNo ratings yet
- Pharmacoeconomics: Health vs. Cost: Netra RisalDocument3 pagesPharmacoeconomics: Health vs. Cost: Netra RisalNetra RisalNo ratings yet
- 5th Pharmacoeconomics Methods CbaDocument54 pages5th Pharmacoeconomics Methods CbaMaria WongaNo ratings yet
- Unit 3Document41 pagesUnit 3Narrainshree SathiyarajeswaranNo ratings yet
- Mission Hospital: Team 6Document14 pagesMission Hospital: Team 6sanray9No ratings yet
- Public Health, Health Economics: Cost-Effectiveness AnalysisDocument40 pagesPublic Health, Health Economics: Cost-Effectiveness AnalysisHashmithaNo ratings yet
- HECO U4 - Eco EvaluationDocument107 pagesHECO U4 - Eco EvaluationMikee MeladNo ratings yet
- Health EconomicsDocument39 pagesHealth EconomicsEster JohannesNo ratings yet
- Community Medicine 2.05 Health-Economics-Dr.-BrizuelaDocument7 pagesCommunity Medicine 2.05 Health-Economics-Dr.-BrizuelaJoher Mendez100% (1)
- PharmacoeconomicsDocument21 pagesPharmacoeconomicsSanthosh KumarNo ratings yet
- Part V: Cost-Effectiveness Analysis: Outcomes in Natural Units: The Fifth of A Five-Part SeriesDocument52 pagesPart V: Cost-Effectiveness Analysis: Outcomes in Natural Units: The Fifth of A Five-Part SeriespatriciavfreitasNo ratings yet
- Rascati Untuk Kuliah Chapter 2Document16 pagesRascati Untuk Kuliah Chapter 2DALI SAPARI 2021No ratings yet
- Economic Evidence For Evidence-Based PracticeDocument6 pagesEconomic Evidence For Evidence-Based PracticeHenri Perwira NegaraNo ratings yet
- Cost Outcome Analysis MillerDocument6 pagesCost Outcome Analysis MillerVarun SoganiNo ratings yet
- ACCT 433 - Role-Playing Assessment RubricDocument5 pagesACCT 433 - Role-Playing Assessment Rubricwafa aljuaidNo ratings yet
- 809kW Marine Propulsion Engine SpecificationsDocument2 pages809kW Marine Propulsion Engine SpecificationsRoberto StepankowskyNo ratings yet
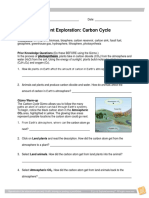
- Carbon Cycle SEDocument7 pagesCarbon Cycle SEAlex0% (3)
- 23rd India Conference of WAVES First AnnouncementDocument1 page23rd India Conference of WAVES First AnnouncementParan GoswamiNo ratings yet
- Creating and Opening WorkbooksDocument20 pagesCreating and Opening WorkbooksCon SiosonNo ratings yet
- How To Knit SocksDocument10 pagesHow To Knit SocksHolly Robles100% (1)
- Nurarihyon No Mago Season 3 Sub Indo PDFDocument3 pagesNurarihyon No Mago Season 3 Sub Indo PDFLgn StruggleNo ratings yet
- Combined Orders (SAP Library - Production Planning and Control)Document3 pagesCombined Orders (SAP Library - Production Planning and Control)Rashid KhanNo ratings yet
- Class 11 Constitutional Law Model QuestionDocument3 pagesClass 11 Constitutional Law Model QuestionanuNo ratings yet
- RC21 ServiceDocument32 pagesRC21 ServiceMuhammedNo ratings yet
- Unsettling Definitions of QualDocument8 pagesUnsettling Definitions of QualJIANING ZHUNo ratings yet
- On January 2 2014 P Company A U S Based Company AcquiredDocument1 pageOn January 2 2014 P Company A U S Based Company AcquiredMuhammad ShahidNo ratings yet
- Encyclopedia of Big Data PDFDocument338 pagesEncyclopedia of Big Data PDFAmit Singh0% (1)
- Definition (Art. 1458)Document10 pagesDefinition (Art. 1458)Fatima SladjannaNo ratings yet
- Analysis of Real Estate Investment at Navasari - BBA Finance Summer Training Project ReportDocument60 pagesAnalysis of Real Estate Investment at Navasari - BBA Finance Summer Training Project ReportPrafull shekhar RojekarNo ratings yet
- United States Bankruptcy Court Eastern District of Michigan Southern DivisionDocument14 pagesUnited States Bankruptcy Court Eastern District of Michigan Southern DivisionChapter 11 DocketsNo ratings yet
- A Review of Solar Photovoltaic System Maintenance StrategiesDocument8 pagesA Review of Solar Photovoltaic System Maintenance StrategiessamNo ratings yet
- SBI PO Exam Call LetterDocument2 pagesSBI PO Exam Call LetterswaroopbhujbalNo ratings yet
- Distillation TypesDocument34 pagesDistillation TypesJoshua Johnson100% (1)
- Unit 1.3 Practice TestDocument16 pagesUnit 1.3 Practice TestYoann DanionNo ratings yet
- BCom Seminar Topics Professors Economics CommerceDocument3 pagesBCom Seminar Topics Professors Economics CommerceShaifali ChauhanNo ratings yet
- Tcds Easa A 359 Dornier 228 Issue 7Document53 pagesTcds Easa A 359 Dornier 228 Issue 7INFO WORKLINKNo ratings yet
- Stability and Development StrategyDocument34 pagesStability and Development StrategySudan North-South Border InitiativeNo ratings yet
- Philips Gemini TF 64 Preferred Room LayoutDocument3 pagesPhilips Gemini TF 64 Preferred Room Layoutahmed_galal_waly1056No ratings yet
- A European Call Option Gives A Person The Right ToDocument1 pageA European Call Option Gives A Person The Right ToAmit PandeyNo ratings yet
- Ielts Vocabulary 1Document2 pagesIelts Vocabulary 1Rizki SalamiNo ratings yet
- PatentDocument4 pagesPatentuser anonymousNo ratings yet
- Product Specifications Product Specifications: SBNHH SBNHH - 1D45C 1D45C - SR SRDocument6 pagesProduct Specifications Product Specifications: SBNHH SBNHH - 1D45C 1D45C - SR SRjorgeerestrepoNo ratings yet
- Flowshield ESD ConductiveDocument2 pagesFlowshield ESD ConductiveRamkumar KumaresanNo ratings yet