You might also like
- NsaidDocument29 pagesNsaidAnonymous vMjb3lQOPoNo ratings yet
- Adrenal FatigueDocument40 pagesAdrenal FatigueNimmi Nims67% (3)
- Adrenocorticoids & Their Physiologic EffectsDocument77 pagesAdrenocorticoids & Their Physiologic EffectsSamson100% (1)
- Soap NotesDocument7 pagesSoap NotesCharles Ravan80% (5)
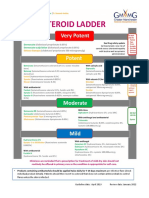
- GM Steroid LadderDocument2 pagesGM Steroid LadderRenee McGuinnessNo ratings yet
- Nsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyDocument65 pagesNsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyYousef JafarNo ratings yet
- NsaidDocument29 pagesNsaidEditya Apriliani100% (1)
- Analgegics & Anti Inflammatories in OS-Dr - siddHARTHDocument46 pagesAnalgegics & Anti Inflammatories in OS-Dr - siddHARTHSiddharth DhanarajNo ratings yet
- Drug Study MMMCDocument14 pagesDrug Study MMMCKathleen Pagulayan Intalan-GloriosoNo ratings yet
- Case Study Addison's Disease Part 1Document27 pagesCase Study Addison's Disease Part 1Whitney PierreNo ratings yet
- FAR 381 - NSAIDs - 2018 - Lecture - UploadDocument51 pagesFAR 381 - NSAIDs - 2018 - Lecture - UploadHuzaifa KhanNo ratings yet
- Analgesic and Anti-Inflammatory Drugs ClassificationDocument64 pagesAnalgesic and Anti-Inflammatory Drugs ClassificationSusy MariyatiNo ratings yet
- Analgesic and Nsaids: Dr. Budhi Setiawan, M.Kes PharmacologyDocument25 pagesAnalgesic and Nsaids: Dr. Budhi Setiawan, M.Kes PharmacologyAyuNo ratings yet
- Obat Anti Inflamasi: Dr. Rohmania SetiariniDocument62 pagesObat Anti Inflamasi: Dr. Rohmania SetiariniafraxyzNo ratings yet
- Anti-Inflammatory, Anti-Arthritis, and Related AgentsDocument22 pagesAnti-Inflammatory, Anti-Arthritis, and Related AgentsMarjolene PudaderaNo ratings yet
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)Document35 pagesNonsteroidal Anti-Inflammatory Drugs (NSAIDs)Areesha ANo ratings yet
- Nsaidsacetaminophen 190220064047Document32 pagesNsaidsacetaminophen 190220064047AugustinoNo ratings yet
- Anti-Inflammatory Drugs.Document48 pagesAnti-Inflammatory Drugs.Amir OnlineNo ratings yet
- Anti-Inflammatory DrugsDocument36 pagesAnti-Inflammatory Drugsnezifzenu2023No ratings yet
- Antiinflammatory Antirheumatic Antigout DrugsDocument22 pagesAntiinflammatory Antirheumatic Antigout DrugsGracia Dela CruzNo ratings yet
- NSAIDsDocument27 pagesNSAIDsshatz_014No ratings yet
- Group 3 AntiinflammatoryDocument83 pagesGroup 3 AntiinflammatoryJesseleAikaAraisNo ratings yet
- Analgesic and Nsaids: Dr. Budhi Setiawan, M.Kes PharmacologyDocument24 pagesAnalgesic and Nsaids: Dr. Budhi Setiawan, M.Kes PharmacologyErwin BawonoNo ratings yet
- CorticosteroidsDocument40 pagesCorticosteroidsBusy worldNo ratings yet
- NsaidDocument51 pagesNsaidDebasis Sahoo100% (1)
- Corticosteroids: Saitoti S. Clinical Pharmacologist UdomDocument33 pagesCorticosteroids: Saitoti S. Clinical Pharmacologist UdomZabron LuhendeNo ratings yet
- Nsaids: On Teroidal Nti Nflammatory RugDocument61 pagesNsaids: On Teroidal Nti Nflammatory RugNdayishimiye ErnestNo ratings yet
- Analgesik: Chenny, Dr. Bagian Farmakologi Fakultas Kedokteran Universitas Wijaya Kusuma SurabayaDocument37 pagesAnalgesik: Chenny, Dr. Bagian Farmakologi Fakultas Kedokteran Universitas Wijaya Kusuma SurabayaWanda Puspita SariNo ratings yet
- Presentation Nadi and DanyDocument7 pagesPresentation Nadi and DanyFadel AhdabNo ratings yet
- Adrenal DisordersDocument26 pagesAdrenal DisordersAsif Ali LashariNo ratings yet
- Nonsteroidal Antiinflammatory Drugs and Antipyretic-AnalgesicsDocument49 pagesNonsteroidal Antiinflammatory Drugs and Antipyretic-AnalgesicsShivsharanNo ratings yet
- NSAIDSDocument19 pagesNSAIDSDonna Kelly DuranNo ratings yet
- NSAIDs: Mechanisms, Effects and Classification in 40 CharactersDocument6 pagesNSAIDs: Mechanisms, Effects and Classification in 40 Charactersmariam_asif_5No ratings yet
- Nonsteroidal Antiinflammatory Drugs and Antipyretic - AnalgesicsDocument28 pagesNonsteroidal Antiinflammatory Drugs and Antipyretic - AnalgesicsJasveen SawhneyNo ratings yet
- CorticosteroidsDocument42 pagesCorticosteroidsejiNo ratings yet
- Gout Presentation Group 2 Defines Metabolic Disorder and ManagementDocument10 pagesGout Presentation Group 2 Defines Metabolic Disorder and ManagementVon Valentine MhuteNo ratings yet
- Inflammation and Anti-Inflammatory DrugsDocument30 pagesInflammation and Anti-Inflammatory DrugsYulia KasihNo ratings yet
- 5 - Adrenal Glands (Adrenocorticoids)Document37 pages5 - Adrenal Glands (Adrenocorticoids)Dr. SaniaNo ratings yet
- Adrenocorticosteroid DrugsDocument22 pagesAdrenocorticosteroid DrugspatiemukokotaNo ratings yet
- BP503T - 15 NsaidsDocument36 pagesBP503T - 15 NsaidsVicky VickyNo ratings yet
- Analgesic Drugs: Dr. Jim AmisiDocument65 pagesAnalgesic Drugs: Dr. Jim AmisiMike AnnisNo ratings yet
- Clinical Toxicology: Dep. of Biopharmaceutics and Clinical PharmacyDocument32 pagesClinical Toxicology: Dep. of Biopharmaceutics and Clinical Pharmacymalak amerNo ratings yet
- NsaidDocument23 pagesNsaidArtika Tika ArtikaNo ratings yet
- By Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4Document4 pagesBy Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4ravi2like100% (2)
- Nsaids PresentationDocument84 pagesNsaids PresentationVictoria ChepkorirNo ratings yet
- MCH Unit5NonsteroidalantiinflammatoryagentsDocument40 pagesMCH Unit5Nonsteroidalantiinflammatoryagentsdottommohamedi.120411No ratings yet
- 2020 Drugs On Pain (Analgesics) - DENTISTRYDocument28 pages2020 Drugs On Pain (Analgesics) - DENTISTRYVisayan Alliah GailNo ratings yet
- NSAIDs: Mechanisms, Effects and UsesDocument43 pagesNSAIDs: Mechanisms, Effects and UsesRitu ShewaniNo ratings yet
- AnalgesicsDocument36 pagesAnalgesicsTakale BuloNo ratings yet
- Treatment of Gout 5Document31 pagesTreatment of Gout 5Jason Roy Edward NathanNo ratings yet
- Non Steroidal Anti Inflammatory Drugs: NsaidsDocument58 pagesNon Steroidal Anti Inflammatory Drugs: NsaidsmahamoudNo ratings yet
- NsaidDocument31 pagesNsaidDr. Hadia NadeemNo ratings yet
- Anti InflammatoryDocument49 pagesAnti InflammatoryMuhammad Shahid BilalNo ratings yet
- 11 28 04 Anti InflammatoryDocument36 pages11 28 04 Anti InflammatorykitsilcNo ratings yet
- Farmakologi Hormon AdrenalDocument17 pagesFarmakologi Hormon AdrenalNana NurhasanahNo ratings yet
- Musculoskeletal DrugsDocument29 pagesMusculoskeletal DrugsjanulNo ratings yet
- Anti Inflammatory DrugsDocument44 pagesAnti Inflammatory DrugsARikoRudyNo ratings yet
- Pharmacotherapy of Musculo-Skeletal, Joints and Bone ProblemsDocument14 pagesPharmacotherapy of Musculo-Skeletal, Joints and Bone ProblemsfateeeNo ratings yet
- SAQ - NSAIDS Mechanism and Side Effect 180209Document6 pagesSAQ - NSAIDS Mechanism and Side Effect 180209anaeshkl100% (1)
- Chapter 24 and 25: Anti-Inflammatories and Analgesics: Jessica Hudson MSN RN Spring 2021Document48 pagesChapter 24 and 25: Anti-Inflammatories and Analgesics: Jessica Hudson MSN RN Spring 2021Karina IvanchenkoNo ratings yet
- Khatib - Anti-Asthma-CorticosteroidsDocument16 pagesKhatib - Anti-Asthma-CorticosteroidsPrabhmeet GroverNo ratings yet
- Non-Steroidal Anti-Inflammatory Drugs (Nsaids) : Dr. Nishant B. BhansaliDocument24 pagesNon-Steroidal Anti-Inflammatory Drugs (Nsaids) : Dr. Nishant B. Bhansaliankit ahirNo ratings yet
- M5 Lesson 2 - AnalgesicsDocument72 pagesM5 Lesson 2 - AnalgesicsClaire Marie AlvaranNo ratings yet
- Corticotropin and Adrenal Corticosteroids: DR - Dr. Asep Sukohar, M.Kes Bagian Farmakologi Dan Terapi FK UnilaDocument31 pagesCorticotropin and Adrenal Corticosteroids: DR - Dr. Asep Sukohar, M.Kes Bagian Farmakologi Dan Terapi FK UnilaArifah Afkar FadilahNo ratings yet
- Voucher-DE SATRIA WIFI-Rp.-2.000 - 8-JAM-vc-877-12.17.20Document1 pageVoucher-DE SATRIA WIFI-Rp.-2.000 - 8-JAM-vc-877-12.17.20Darma Satria0% (1)
- Satria PrintrDocument2 pagesSatria PrintrDarma Satria0% (1)
- 1000 JNGN D Print NitipDocument1 page1000 JNGN D Print NitipDarma SatriaNo ratings yet
- Data Bantuan Kuota (Ners)Document6 pagesData Bantuan Kuota (Ners)Darma SatriaNo ratings yet
- DIURETICS - Dr. AgungDocument14 pagesDIURETICS - Dr. AgungDarma SatriaNo ratings yet
- Public WiFi Rental by the Hour, Day in IndonesiaDocument1 pagePublic WiFi Rental by the Hour, Day in IndonesiaDarma SatriaNo ratings yet
- I Gede Darma Satria Utama Diarrhoea ArticleDocument1 pageI Gede Darma Satria Utama Diarrhoea ArticleDarma SatriaNo ratings yet
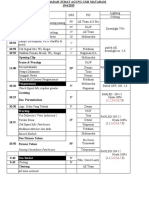
- RUN DOWN IBADAH JUMAT AGUNG GMS MATARAMDocument2 pagesRUN DOWN IBADAH JUMAT AGUNG GMS MATARAMDarma SatriaNo ratings yet
- Diagnosis and Treatment of Keloids and Hypertrophic Scars - Japan Scar Workshop Consensus Document 2018Document40 pagesDiagnosis and Treatment of Keloids and Hypertrophic Scars - Japan Scar Workshop Consensus Document 2018ShintaNo ratings yet
- Flixonase-Nasule-Drops Pi 004 04 Draft-CleanDocument10 pagesFlixonase-Nasule-Drops Pi 004 04 Draft-CleanNisrin SaadNo ratings yet
- Form Pg-Sga PDFDocument2 pagesForm Pg-Sga PDFzain syalsabila0% (1)
- Clinico-Epidemiological Study of Topical Steroid Damaged Face in A Tertiary Care HospitalDocument11 pagesClinico-Epidemiological Study of Topical Steroid Damaged Face in A Tertiary Care HospitalIJAR JOURNALNo ratings yet
- Florinef SPCDocument7 pagesFlorinef SPCJohn GoulianosNo ratings yet
- Uso de Esteroides en AnestesiaDocument7 pagesUso de Esteroides en AnestesiatitinodeNo ratings yet
- ACOG Practice Bulletin - Number 90 - Asthma in PregnancyDocument8 pagesACOG Practice Bulletin - Number 90 - Asthma in PregnancyDecha SaechoenNo ratings yet
- NCLEX Review Cardiovascular QuizDocument17 pagesNCLEX Review Cardiovascular Quizdany tesemaNo ratings yet
- Adult ( 18 Years) Asthma Quick Reference Guide (Update Nov 2017)Document2 pagesAdult ( 18 Years) Asthma Quick Reference Guide (Update Nov 2017)Nerissa Neri NatataNo ratings yet
- Crema Eumovate 0,05%Document7 pagesCrema Eumovate 0,05%Jorge AsimbayaNo ratings yet
- HydrocortisoneDocument1 pageHydrocortisoneRoch OconerNo ratings yet
- Corticosteroid Injections For Painful Shoulder:: A Meta-AnalysisDocument5 pagesCorticosteroid Injections For Painful Shoulder:: A Meta-AnalysismissrinwaNo ratings yet
- Topical Steroids (Sep 16)Document7 pagesTopical Steroids (Sep 16)lalaNo ratings yet
- 1210SDocument152 pages1210SChoon Fong LeeNo ratings yet
- Dafpus SGB 20Document32 pagesDafpus SGB 20Anggie Pradetya MaharaniNo ratings yet
- Glucocorticoids: Synthesis, Mechanisms, Uses and Side EffectsDocument48 pagesGlucocorticoids: Synthesis, Mechanisms, Uses and Side EffectscatherinaywNo ratings yet
- BMRB Entry 6269Document29 pagesBMRB Entry 6269Putu MahendraNo ratings yet
- Steroid PaperDocument16 pagesSteroid PaperkhyatisethiaNo ratings yet
- Efficacy of Dexamethasone Versus Fluticasone Nasal Sprays in Postoperative Patients With Chronic Rhinosinusitis With Nasal PolypsDocument5 pagesEfficacy of Dexamethasone Versus Fluticasone Nasal Sprays in Postoperative Patients With Chronic Rhinosinusitis With Nasal PolypsandiniNo ratings yet
- Anabolic Steroids HandoutDocument4 pagesAnabolic Steroids HandoutDiana AstriaNo ratings yet
- BetamethasonaDocument10 pagesBetamethasonaJuan PerezNo ratings yet
- Dara Mola 2016Document5 pagesDara Mola 2016andiniNo ratings yet
- All DrugsDocument482 pagesAll DrugsJessica IbañezNo ratings yet
- Flutivate Skin Cream 1. Generic Name: For The Use Only of Registered Medical Practitioners or A Hospital or A LaboratoryDocument11 pagesFlutivate Skin Cream 1. Generic Name: For The Use Only of Registered Medical Practitioners or A Hospital or A LaboratoryManas MishraNo ratings yet
- Classification of Topical Corticosteroids (WHO)Document2 pagesClassification of Topical Corticosteroids (WHO)Sandy GunawanNo ratings yet