You might also like
- Solvents and Their Nomenclauture PDFDocument10 pagesSolvents and Their Nomenclauture PDFAashish GauravNo ratings yet
- Hematemesis, Melena, HematoscheziaDocument48 pagesHematemesis, Melena, HematoscheziaSyarifah FauziahNo ratings yet
- Introduction, Concepts, Scope of Community Health NursingDocument32 pagesIntroduction, Concepts, Scope of Community Health Nursingmuthukumar82% (28)
- InfluencerDocument198 pagesInfluencerAkanksha SethiNo ratings yet
- Acute Pulmonary Embolism Final YearDocument52 pagesAcute Pulmonary Embolism Final YearUzma BanoNo ratings yet
- Radiant Heating and Cooling SystemDocument8 pagesRadiant Heating and Cooling SystemLaurentiuNo ratings yet
- Ball ValveDocument12 pagesBall ValveIdabaNo ratings yet
- Presented By: Dr. Siddhant Singh Moderator: Prof. Dr. Sanjay Kala (MS)Document100 pagesPresented By: Dr. Siddhant Singh Moderator: Prof. Dr. Sanjay Kala (MS)Sid Sid100% (2)
- 09 Endoscopia Interventionala PDFDocument76 pages09 Endoscopia Interventionala PDFDark1oneNo ratings yet
- Welding Cost Optimization with GMAWDocument6 pagesWelding Cost Optimization with GMAWratneshkumar2004No ratings yet
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- 9211 4 PR PE Utility Industry Low Product Range 2017Document226 pages9211 4 PR PE Utility Industry Low Product Range 2017Soporte SyeNo ratings yet
- GI Bleeding - NursesDocument71 pagesGI Bleeding - Nursesapi-3760283100% (6)
- A350 XWB Training Brochure PDFDocument8 pagesA350 XWB Training Brochure PDFBertrand100% (1)
- Approach To GI BleedDocument97 pagesApproach To GI BleedPankaj IngleNo ratings yet
- Alejandra Vélez Perea Res. Ginecología y ObstetriciaDocument71 pagesAlejandra Vélez Perea Res. Ginecología y ObstetriciaMagic_OverNo ratings yet
- The Influence of Spleen On Portal HemodynamicsDocument1 pageThe Influence of Spleen On Portal HemodynamicsdenisegmeloNo ratings yet
- Rev-Inhibitor Manado 2017Document37 pagesRev-Inhibitor Manado 2017Utari UbNo ratings yet
- IPD - Kelas AC - Perdarahan Sal. Cerna - Dr. Hery Djagat - 28 Agustus 2018Document75 pagesIPD - Kelas AC - Perdarahan Sal. Cerna - Dr. Hery Djagat - 28 Agustus 2018evanoNo ratings yet
- Perdarahan Saluran Cerna: Oleh: Salman Paris.HDocument69 pagesPerdarahan Saluran Cerna: Oleh: Salman Paris.HaulianaNo ratings yet
- Upper Gastrointestinal Bleeding: (UGIB)Document39 pagesUpper Gastrointestinal Bleeding: (UGIB)api-19916399No ratings yet
- Gastrointestinal Bleeding: Dr. Székely Hajnal 2nd Department of Internal Medicine 2015/16-IDocument74 pagesGastrointestinal Bleeding: Dr. Székely Hajnal 2nd Department of Internal Medicine 2015/16-ISutisna NisaNo ratings yet
- Management of Variceal HemorrhageDocument84 pagesManagement of Variceal HemorrhageDenata PrabhasiwiNo ratings yet
- Management of Variceal HemorrhageDocument84 pagesManagement of Variceal HemorrhageFerry SahraNo ratings yet
- Clinical management of Covid19 updateDocument57 pagesClinical management of Covid19 updateJashveerBediNo ratings yet
- Pulmonology algorithms and pneumonia risk factorsDocument117 pagesPulmonology algorithms and pneumonia risk factorsEm TimbolNo ratings yet
- Sepsisu L La Copil: Sef Lucrari Dr. Adrian Craciun Clinica I Pediat Rie TimisoaraDocument25 pagesSepsisu L La Copil: Sef Lucrari Dr. Adrian Craciun Clinica I Pediat Rie TimisoaraAdrian CraciunNo ratings yet
- Pleural Diseases: Farhad Mazdisnian, MD, FCCP Pulmonary and Critical Care Medicine Va Long Beach Medical CenterDocument46 pagesPleural Diseases: Farhad Mazdisnian, MD, FCCP Pulmonary and Critical Care Medicine Va Long Beach Medical CenterderereyNo ratings yet
- Peptic Ulcer Disease and H pylori Pathogenesis TreatmentDocument19 pagesPeptic Ulcer Disease and H pylori Pathogenesis TreatmentKiara GovenderNo ratings yet
- Acute Upper GI BleedingDocument31 pagesAcute Upper GI BleedingEusebius01No ratings yet
- Simposium Iii. 2. Guch. Dr. L. Krisdinarti SPPD SPJPK PDFDocument33 pagesSimposium Iii. 2. Guch. Dr. L. Krisdinarti SPPD SPJPK PDFbagus krisnaNo ratings yet
- Tips to Save Septic Patients in Emergency DepartmentsDocument109 pagesTips to Save Septic Patients in Emergency DepartmentsaliNo ratings yet
- Liver Disease: Understanding Cirrhosis Causes, Stages and TreatmentDocument48 pagesLiver Disease: Understanding Cirrhosis Causes, Stages and TreatmentNuthahai SimangernNo ratings yet
- Downloadfile 5Document51 pagesDownloadfile 5Faheem Ul HasanNo ratings yet
- Weledji 2020Document7 pagesWeledji 2020Felipe CarmonaNo ratings yet
- Treatment and Complications of Chronic Liver DiseaseDocument40 pagesTreatment and Complications of Chronic Liver DiseaseRisydaMKhNo ratings yet
- Non-Variceal Upper GI Bleeding GuideDocument34 pagesNon-Variceal Upper GI Bleeding GuideChe Ainil ZainodinNo ratings yet
- The Need of Anti Hepatic Fibrosis Cirrhosis Treatment For Chronic Hepatitis CHB CHC Ash Nash Etc Including For Those With Normal AltDocument27 pagesThe Need of Anti Hepatic Fibrosis Cirrhosis Treatment For Chronic Hepatitis CHB CHC Ash Nash Etc Including For Those With Normal AlttrimardiyanaisyanNo ratings yet
- Update on clinical management of Covid19Document49 pagesUpdate on clinical management of Covid19anisNo ratings yet
- Drug Monograph ExampleDocument6 pagesDrug Monograph ExampleAaltiyaNo ratings yet
- NEONATOLOGI - Sepsis Neonatorum + TTN + Neo PneumoniaDocument18 pagesNEONATOLOGI - Sepsis Neonatorum + TTN + Neo PneumoniaGaluh Martin MaytasariNo ratings yet
- Urinary Tract Infection: Case ReportDocument16 pagesUrinary Tract Infection: Case ReportAulia RahmanNo ratings yet
- Suggested Algorithm For Patients With Acute Upper .: BleedingDocument4 pagesSuggested Algorithm For Patients With Acute Upper .: BleedingMimi Marjorie TecNo ratings yet
- Inpatient Management of Patients With Liver CirrhosisDocument52 pagesInpatient Management of Patients With Liver CirrhosisSophia DevtaNo ratings yet
- Maternal Collapse Due To PEDocument57 pagesMaternal Collapse Due To PEAnil JasaniNo ratings yet
- Agnes Lee Thrombosis PresentationDocument37 pagesAgnes Lee Thrombosis Presentationari naNo ratings yet
- NC InfeksiAndi Asriel DBDDocument20 pagesNC InfeksiAndi Asriel DBDeunike jaequelineNo ratings yet
- PancreatitisDocument45 pagesPancreatitisFernando ArancibiaNo ratings yet
- Pragmatic Use of NOACDocument38 pagesPragmatic Use of NOACDr. Pradip MateNo ratings yet
- 5 - 20161121albumin Replacement in SepsisDocument47 pages5 - 20161121albumin Replacement in Sepsisfareehakanwar93No ratings yet
- Urinary Tract Infection: Case ReportDocument17 pagesUrinary Tract Infection: Case ReportjoyNo ratings yet
- Rivaroxaban For VTEDocument35 pagesRivaroxaban For VTENur Sabriany LihawaNo ratings yet
- VirologyDocument31 pagesVirologyDonzzkie DonNo ratings yet
- Deep Vein Thrombosis / Pulmonary EmbolismDocument55 pagesDeep Vein Thrombosis / Pulmonary EmbolismSenti AnnamalaiNo ratings yet
- NC CARDIO - RanggaDocument21 pagesNC CARDIO - RanggaRima KhairunnisaNo ratings yet
- Gastrointestinal Bleeding: Rajeev Jain, M.DDocument51 pagesGastrointestinal Bleeding: Rajeev Jain, M.DNovita AnjaniNo ratings yet
- Adhesive Small Bowel Obstruction: Leslie Kobayashi Trauma Conference 2013Document56 pagesAdhesive Small Bowel Obstruction: Leslie Kobayashi Trauma Conference 2013Ananda RizkiNo ratings yet
- 12-Liver Cirrhosis 2012Document73 pages12-Liver Cirrhosis 2012nadiaNo ratings yet
- Bacterial MeningitisDocument43 pagesBacterial MeningitisEarl MARKNo ratings yet
- Joe Carcillo - Hemodynamic Managemnet in Peidtric SepsisDocument92 pagesJoe Carcillo - Hemodynamic Managemnet in Peidtric SepsisMega SeptianaNo ratings yet
- Dr. Saut Nababan, SP - PD, PH.D: Riwayat PendidikanDocument20 pagesDr. Saut Nababan, SP - PD, PH.D: Riwayat PendidikanRini WidyantariNo ratings yet
- Managing Diabetic Foot Complications and Insulin RequirementsDocument22 pagesManaging Diabetic Foot Complications and Insulin RequirementsJude Micko Bunyi Alipit100% (1)
- NC Muh. YahyaDocument19 pagesNC Muh. YahyaHardiyanti HermanNo ratings yet
- Major Liver Resection PIN IKABDI Bali 4 Okt 2014 711DFDocument32 pagesMajor Liver Resection PIN IKABDI Bali 4 Okt 2014 711DFElandha PutriNo ratings yet
- NC - Immanuel Ata TuruDocument20 pagesNC - Immanuel Ata TuruDodi DiNo ratings yet
- Anticoagulation TherapyFrom EverandAnticoagulation TherapyJoe F. LauNo ratings yet
- Variceal HemorrhageFrom EverandVariceal HemorrhageRoberto de FranchisNo ratings yet
- Klasifikasi Tindakan Bedah Digestif Update 20 Juni 2022 (BPJS)Document7 pagesKlasifikasi Tindakan Bedah Digestif Update 20 Juni 2022 (BPJS)Eko RistiyantoNo ratings yet
- OUTPUTDocument65 pagesOUTPUTEko RistiyantoNo ratings yet
- Internal Herniation Through Foramen of Winslow: A Case ReportDocument3 pagesInternal Herniation Through Foramen of Winslow: A Case ReportEko RistiyantoNo ratings yet
- Grafik Kuman TPPDocument2 pagesGrafik Kuman TPPEko RistiyantoNo ratings yet
- License AgreementDocument1 pageLicense AgreementEko RistiyantoNo ratings yet
- New Ropanasuri Journal of Surgery Form For Disclosure of Potential Conflicts of InterestDocument3 pagesNew Ropanasuri Journal of Surgery Form For Disclosure of Potential Conflicts of InterestEko RistiyantoNo ratings yet
- Survival Analysis of Palliative Surgery of Advanced Stage Periampullary Cancer PDFDocument6 pagesSurvival Analysis of Palliative Surgery of Advanced Stage Periampullary Cancer PDFEko RistiyantoNo ratings yet
- 702 1383 1 PB PDFDocument7 pages702 1383 1 PB PDFEko RistiyantoNo ratings yet
- Excli 17 159 PDFDocument10 pagesExcli 17 159 PDFEko RistiyantoNo ratings yet
- Simanjuntak 2018 J. Phys. Conf. Ser. 1073 042021 PDFDocument8 pagesSimanjuntak 2018 J. Phys. Conf. Ser. 1073 042021 PDFEko RistiyantoNo ratings yet
- Nutrition Services Screening Assessment (NSSA) SebagaiDocument8 pagesNutrition Services Screening Assessment (NSSA) SebagaiEko RistiyantoNo ratings yet
- Mco 03 03 0699 PDFDocument7 pagesMco 03 03 0699 PDFEko RistiyantoNo ratings yet
- 1775 PDFDocument7 pages1775 PDFEko RistiyantoNo ratings yet
- Global Assessment (PG-SGA) Berhubungan Dengan Asupan ZatDocument5 pagesGlobal Assessment (PG-SGA) Berhubungan Dengan Asupan ZatDea SaptanovaNo ratings yet
- Herna Through Winslow Foramen A Case ReportDocument3 pagesHerna Through Winslow Foramen A Case ReportEko RistiyantoNo ratings yet
- s12935 019 1091 8 PDFDocument13 pagess12935 019 1091 8 PDFEko RistiyantoNo ratings yet
- Subjective Global Assessment Form: Medical HistoryDocument2 pagesSubjective Global Assessment Form: Medical Historynadia susiyanaNo ratings yet
- Tumors of The Amputla: Pathogenesis and Prognostic Factors: PathogensDocument3 pagesTumors of The Amputla: Pathogenesis and Prognostic Factors: PathogensEko RistiyantoNo ratings yet
- Liver TransplantDocument13 pagesLiver TransplantEko RistiyantoNo ratings yet
- Perbaikan Tugas Genetka Eko Ristiyanto Bedah Digestif Caroli Deseas GoleDocument18 pagesPerbaikan Tugas Genetka Eko Ristiyanto Bedah Digestif Caroli Deseas GoleEko RistiyantoNo ratings yet
- Current Trends in Management of Acute Pancreatitis A ReviewDocument7 pagesCurrent Trends in Management of Acute Pancreatitis A ReviewPaul HartingNo ratings yet
- Kronik PankreatitisDocument41 pagesKronik PankreatitisEko RistiyantoNo ratings yet
- PancreatitisDocument20 pagesPancreatitisViviana CarimanNo ratings yet
- Modern Control Systems Linear Approximation Laplace TransformDocument3 pagesModern Control Systems Linear Approximation Laplace TransformramNo ratings yet
- Draytek 2 Cisco VPNDocument8 pagesDraytek 2 Cisco VPNMarco ManzanoNo ratings yet
- Plan Test Strategy for Flight Search WebsiteDocument13 pagesPlan Test Strategy for Flight Search WebsiteНаталья ПримаNo ratings yet
- 10 - A TFT-LCD Source-Driver IC With Charge-Recycling TechniqueDocument11 pages10 - A TFT-LCD Source-Driver IC With Charge-Recycling Techniquematwan29No ratings yet
- HyungJae Yang Sound Water EnvironmentDocument25 pagesHyungJae Yang Sound Water EnvironmentPepeNo ratings yet
- Evolution of Arbitration in IndiaDocument8 pagesEvolution of Arbitration in IndiaPururaj AggarwalNo ratings yet
- السيرة الذاتيةDocument1 pageالسيرة الذاتيةYounesNo ratings yet
- Objective: Ofdm ModulationDocument10 pagesObjective: Ofdm ModulationxxNo ratings yet
- GPS Consent and TrackingDocument3 pagesGPS Consent and TrackingJoel KionisalaNo ratings yet
- AI Story WritermnfyaDocument2 pagesAI Story Writermnfyafrenchrugby98No ratings yet
- Stolle Cupping Systems: ConnectingDocument2 pagesStolle Cupping Systems: ConnectingHieu NguyenNo ratings yet
- North American Free Trade Agreement: Prof. MakhmoorDocument15 pagesNorth American Free Trade Agreement: Prof. MakhmoorShikha ShuklaNo ratings yet
- Literature Review On School AdministrationDocument6 pagesLiterature Review On School Administrationea7sfn0f100% (1)
- Office & Branches: Head Office PT Indosat Mega Media (IM2)Document4 pagesOffice & Branches: Head Office PT Indosat Mega Media (IM2)satriamesumNo ratings yet
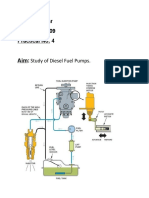
- Study of Diesel Fuel Pumps ComponentsDocument6 pagesStudy of Diesel Fuel Pumps ComponentsPro GamerssNo ratings yet
- Model checking flight control systems experienceDocument11 pagesModel checking flight control systems experienceCORAL ALONSONo ratings yet
- FoCal Multi-class Toolkit GuideDocument32 pagesFoCal Multi-class Toolkit Guidethyagosmesme100% (1)
- Mitchell Board of Education June 26 Meeting AgendaDocument33 pagesMitchell Board of Education June 26 Meeting AgendainforumdocsNo ratings yet
- Bulk PricesDocument2 pagesBulk PricesMega Byte0% (1)
- Working Capital Management OF: Submitted by Priya BanerjeeDocument102 pagesWorking Capital Management OF: Submitted by Priya BanerjeeSushmita BarlaNo ratings yet
- IELTS PART 1 (Autoguardado)Document8 pagesIELTS PART 1 (Autoguardado)CARLOS CAICEDONo ratings yet
- 2016 Students ch04 - Lovelock - Developing Service Products - 6e - STUDENTDocument36 pages2016 Students ch04 - Lovelock - Developing Service Products - 6e - STUDENTbold onyxNo ratings yet