You might also like
- Physiology of Drowning PDFDocument63 pagesPhysiology of Drowning PDFPeter PhelpsNo ratings yet
- Environmental Emergencies ParamedicDocument90 pagesEnvironmental Emergencies ParamedicPaulhotvw67100% (2)
- ECHO MASTERCLASS: A GUIDE TO ACCURATELY ASSESSING HEART VALVE DISEASEDocument136 pagesECHO MASTERCLASS: A GUIDE TO ACCURATELY ASSESSING HEART VALVE DISEASEVladlena Cucoș-CaraimanNo ratings yet
- Anup Calculation SheetDocument33 pagesAnup Calculation SheetAziz AndriyantoNo ratings yet
- @MBS MedicalBooksStore 2020 HeadDocument238 pages@MBS MedicalBooksStore 2020 HeadtamiNo ratings yet
- Environmental EmergenciesDocument38 pagesEnvironmental EmergenciesIshaBrijeshSharmaNo ratings yet
- Guide to Neurology ClerkshipDocument63 pagesGuide to Neurology ClerkshipShane AllenNo ratings yet
- Electrical Injury: By: Mohd Khairul Izzati OmarDocument28 pagesElectrical Injury: By: Mohd Khairul Izzati OmarInsyirah QalbiNo ratings yet
- Drowning Pathophysiology and Prediction of OutcomeDocument48 pagesDrowning Pathophysiology and Prediction of OutcomeFitri Amelia RizkiNo ratings yet
- Rheumatic Heart DiseaseDocument37 pagesRheumatic Heart Diseasesalman hNo ratings yet
- CPG Labor and Delivery 2015Document78 pagesCPG Labor and Delivery 2015TintalleNo ratings yet
- MCQ exam on pharmacology, medicine and treatmentsDocument10 pagesMCQ exam on pharmacology, medicine and treatmentsعزالدين الطيارNo ratings yet
- Patient Centered Communication Standards (JCAHO)Document102 pagesPatient Centered Communication Standards (JCAHO)kcochran100% (1)
- SOP For Heat Disorders 2016Document13 pagesSOP For Heat Disorders 2016NyanLinKyawNo ratings yet
- Kegawatdaruratan EnvironmentDocument50 pagesKegawatdaruratan EnvironmentdenishNo ratings yet
- Pathophysiology of Septic & Septic Shock, DR Christian A Johannes SpAnDocument56 pagesPathophysiology of Septic & Septic Shock, DR Christian A Johannes SpAnmonicaolivine100% (1)
- Frostbite: Putra Haqiqie Adnantama LubisDocument13 pagesFrostbite: Putra Haqiqie Adnantama LubisKurniadi YusufNo ratings yet
- Environmental Emergencies Heat Exhaustion HeatstrokeDocument6 pagesEnvironmental Emergencies Heat Exhaustion HeatstrokepauchanmnlNo ratings yet
- Nur 111 Session 21 Sas 1Document8 pagesNur 111 Session 21 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Frostbite and HypothermiaDocument43 pagesFrostbite and HypothermiaBlade DarkmanNo ratings yet
- Hyper and HypothermiaDocument4 pagesHyper and HypothermiaSaharAhmadNo ratings yet
- Heat Stroke and Hypothermia: Jagdish Dureja and Harpreet SinghDocument9 pagesHeat Stroke and Hypothermia: Jagdish Dureja and Harpreet SinghHandjar DaNo ratings yet
- 20230923-21444-50guzkDocument6 pages20230923-21444-50guzkEster DuwitNo ratings yet
- Prehospitalresearch - Eu-Case Study 4 HypothermiaDocument10 pagesPrehospitalresearch - Eu-Case Study 4 Hypothermiasultan almehmmadiNo ratings yet
- Therapeutic HypothermiaDocument7 pagesTherapeutic HypothermiaTracyNo ratings yet
- 4 9 Heat Stroke PDFDocument6 pages4 9 Heat Stroke PDFmia nurjanahNo ratings yet
- Diagnosis and Management of Heatstroke: I Gede Yasa AsmaraDocument8 pagesDiagnosis and Management of Heatstroke: I Gede Yasa AsmaraputryaNo ratings yet
- BURNSDocument4 pagesBURNSIlyes FerenczNo ratings yet
- FrostbiteDocument19 pagesFrostbiteKhadim Hussain Shah100% (1)
- Anaesthetic Considerations in Trauma by DR Supria GajendragadkarDocument59 pagesAnaesthetic Considerations in Trauma by DR Supria GajendragadkarcardiacanesthesiaNo ratings yet
- Frost BiteDocument21 pagesFrost BiteNavid KhNo ratings yet
- Frost BiteDocument21 pagesFrost BiteNavid KhNo ratings yet
- Clinical Communications: Skin and Soft Tissue Necrosis From Calcium Chloride in A DeicerDocument4 pagesClinical Communications: Skin and Soft Tissue Necrosis From Calcium Chloride in A Deicerduy NguyễnNo ratings yet
- Hot and Cold Application - PPTX RevisedDocument61 pagesHot and Cold Application - PPTX RevisedMicah HuanNo ratings yet
- Environmental Cold Injury and Illness Prevention PolicyDocument12 pagesEnvironmental Cold Injury and Illness Prevention Policyapi-381026050No ratings yet
- Cold InjuryDocument10 pagesCold Injuryaishaiqbal6789No ratings yet
- A MISLEADING FORM OF IDIOPATHIC CAPILLARY LEAKAGE SYNDROME (CLARKSONS DISEASE): A CASE REPORTDocument5 pagesA MISLEADING FORM OF IDIOPATHIC CAPILLARY LEAKAGE SYNDROME (CLARKSONS DISEASE): A CASE REPORTIJAR JOURNALNo ratings yet
- Kegawatdarutan Mata Dalam Konsep DogaDocument68 pagesKegawatdarutan Mata Dalam Konsep DogaDavi DzikirianNo ratings yet
- Fever 150910135159 Lva1 App6892Document48 pagesFever 150910135159 Lva1 App6892AhteshamNo ratings yet
- Acute Skin Failure: Moderator: DR Girisha Bs By: DR Preethi B NayakDocument52 pagesAcute Skin Failure: Moderator: DR Girisha Bs By: DR Preethi B NayakGreeshmaNo ratings yet
- Cold Injury Management GuideDocument34 pagesCold Injury Management Guidedassdeepak69100% (1)
- Ch14 ClinicalAspectsofFreezingColdInjuryDocument38 pagesCh14 ClinicalAspectsofFreezingColdInjuryLee SmithNo ratings yet
- Cold and Heat Therapy 护理学院朱晓雯(以此版本为准)Document24 pagesCold and Heat Therapy 护理学院朱晓雯(以此版本为准)sargunavalli balrajNo ratings yet
- Bacterial EndocarditisDocument5 pagesBacterial EndocarditisAMOS MELINo ratings yet
- Cardiovascular Diseases 2Document40 pagesCardiovascular Diseases 2Ali MuradNo ratings yet
- Kim 2020Document4 pagesKim 2020Ester DuwitNo ratings yet
- Rheumatic Fever and Heart DiseaseDocument37 pagesRheumatic Fever and Heart Diseasejiregna eticha dakoNo ratings yet
- NCP CnsiDocument2 pagesNCP CnsiJennylyn Barcelona BironNo ratings yet
- Changes After Death 23Document136 pagesChanges After Death 23asifazizhaqueNo ratings yet
- Clinical Communications: Adult: Cold Anaphylaxis: A Case ReportDocument3 pagesClinical Communications: Adult: Cold Anaphylaxis: A Case Reportdesta widayatNo ratings yet
- Burns-Dr. OduorDocument49 pagesBurns-Dr. OduorBrayen WaichigoNo ratings yet
- Traumatic Amputation and Replantation Techniques ExplainedDocument28 pagesTraumatic Amputation and Replantation Techniques ExplainedEka Kristi PermatasariNo ratings yet
- Problem 2 JojoDocument62 pagesProblem 2 JojoWielda MutafadhilahNo ratings yet
- Acute Biologic Crisis - Hand OutDocument48 pagesAcute Biologic Crisis - Hand OutLouis Carlos RoderosNo ratings yet
- 418 m3 Cu13 Clients With Multisystem ProblemsDocument8 pages418 m3 Cu13 Clients With Multisystem ProblemsDanica FrancoNo ratings yet
- Burns Presentation-WPS OfficeDocument41 pagesBurns Presentation-WPS OfficeSobia QasimNo ratings yet
- SIRS, Sepsis, MODS Defined in Critical Care LectureDocument32 pagesSIRS, Sepsis, MODS Defined in Critical Care LecturetotoksaptantoNo ratings yet
- Mechanism of TraumaDocument46 pagesMechanism of TraumauutNo ratings yet
- Emergency Nursing SkillsDocument7 pagesEmergency Nursing SkillsPxPPxH ChanNo ratings yet
- Allergic ConjunctivitisDocument33 pagesAllergic ConjunctivitisNor Faezah Abd HamidNo ratings yet
- ASKEP SHOCK SEPSIS, DISTRIBUTIF & ANAFILAKTIKDocument28 pagesASKEP SHOCK SEPSIS, DISTRIBUTIF & ANAFILAKTIKTomi KurniaNo ratings yet
- Cryosurgery and ElectrosurgeryDocument51 pagesCryosurgery and ElectrosurgeryVeerabhadra RadhakrishnaNo ratings yet
- Valvular Heart Disease: Cardiology Division, Medical Faculty Diponegoro UniversityDocument46 pagesValvular Heart Disease: Cardiology Division, Medical Faculty Diponegoro UniversityChacha TasyaNo ratings yet
- CU. 9 BurnsDocument50 pagesCU. 9 BurnsCechanNo ratings yet
- Temperature Monitoring: Moderator: DR Raktima Anand Presenter: DR Prashanth SDocument36 pagesTemperature Monitoring: Moderator: DR Raktima Anand Presenter: DR Prashanth SprashsubbuNo ratings yet
- Memo Cut Off JMDocument1 pageMemo Cut Off JMAziz AndriyantoNo ratings yet
- SRT Und SpOGDocument2 pagesSRT Und SpOGAziz AndriyantoNo ratings yet
- Manage Frostbite at the EDDocument19 pagesManage Frostbite at the EDAziz AndriyantoNo ratings yet
- Final AnnouncementDocument14 pagesFinal AnnouncementAziz AndriyantoNo ratings yet
- Intensive Insulin Therapy Dr. Hemi, SP - PDDocument10 pagesIntensive Insulin Therapy Dr. Hemi, SP - PDAziz AndriyantoNo ratings yet
- The 2 National Annual Scientific Meeting On Emergency Medicine 2014Document1 pageThe 2 National Annual Scientific Meeting On Emergency Medicine 2014Aziz AndriyantoNo ratings yet
- Snake Antivenom Guide in UKMMCDocument7 pagesSnake Antivenom Guide in UKMMCAziz AndriyantoNo ratings yet
- Clinical Toxicology Toxicant Assesment in Emergency DepartmentDocument44 pagesClinical Toxicology Toxicant Assesment in Emergency DepartmentAziz AndriyantoNo ratings yet
- 2nd National Annual Scientific Meeting on Emergency Medicine 2014Document1 page2nd National Annual Scientific Meeting on Emergency Medicine 2014Aziz AndriyantoNo ratings yet
- OpeningDocument8 pagesOpeningitsuport rsuiiNo ratings yet
- Caustic Agent RevDocument32 pagesCaustic Agent RevAziz AndriyantoNo ratings yet
- HousehoŬdĠPoisoning AbstractDocument1 pageHousehoŬdĠPoisoning AbstractAziz AndriyantoNo ratings yet
- Rev CenterDocument19 pagesRev CenterAziz AndriyantoNo ratings yet
- Caustic Agent RevDocument32 pagesCaustic Agent RevAziz AndriyantoNo ratings yet
- How To Deliver Antiseizure Drugs in Infant & Children - Dr. SuDocument34 pagesHow To Deliver Antiseizure Drugs in Infant & Children - Dr. SuAziz AndriyantoNo ratings yet
- How To Deliver Antiseizure Drugs in Infant & Children - Dr. SuDocument34 pagesHow To Deliver Antiseizure Drugs in Infant & Children - Dr. SuAziz AndriyantoNo ratings yet
- Analgesia and Sedation in ERDocument41 pagesAnalgesia and Sedation in ERAziz AndriyantoNo ratings yet
- Cleaning Mud Mixing Tanks JSADocument7 pagesCleaning Mud Mixing Tanks JSAAziz AndriyantoNo ratings yet
- Dr. Edy F-Edy F, ROSADE Lampung, 2020Document19 pagesDr. Edy F-Edy F, ROSADE Lampung, 2020Aziz AndriyantoNo ratings yet
- EMERGENCY PHYSICIAN CV SUMMARYDocument15 pagesEMERGENCY PHYSICIAN CV SUMMARYAziz AndriyantoNo ratings yet
- DMR 021 - Louisiana - A 2 D - 09 Oct 18Document5 pagesDMR 021 - Louisiana - A 2 D - 09 Oct 18Aziz AndriyantoNo ratings yet
- 2nd National Annual Scientific Meeting on Emergency Medicine 2014Document1 page2nd National Annual Scientific Meeting on Emergency Medicine 2014Aziz AndriyantoNo ratings yet
- Interval Discussion 42in & 26in PhaseDocument3 pagesInterval Discussion 42in & 26in PhaseAziz AndriyantoNo ratings yet
- CamScanner Scans PDFs from PhotosDocument3 pagesCamScanner Scans PDFs from PhotosAziz AndriyantoNo ratings yet
- Lembar Triase PDFDocument3 pagesLembar Triase PDFAziz AndriyantoNo ratings yet
- Jadwal Dokter Umum (Desember 2019) Siap PrintDocument11 pagesJadwal Dokter Umum (Desember 2019) Siap PrintAziz AndriyantoNo ratings yet
- DMR-019 - Louisiana - A-2-D - 07 - Oct-18Document5 pagesDMR-019 - Louisiana - A-2-D - 07 - Oct-18Aziz AndriyantoNo ratings yet
- Strabismus Prevalence and Associated Factors Among Pediatric Patients in Southern Ethiopia: A Cross-Sectional StudyDocument10 pagesStrabismus Prevalence and Associated Factors Among Pediatric Patients in Southern Ethiopia: A Cross-Sectional StudyDenise MacieNo ratings yet
- Worksheet 1 (Before Lec 1) PDFDocument4 pagesWorksheet 1 (Before Lec 1) PDFLei Zaira BiendimaNo ratings yet
- Case Pres TamparanDocument22 pagesCase Pres TamparanAlano S. LimgasNo ratings yet
- Bacterial Meningitis Causes, Symptoms, and Diagnosis in Children Over 1 MonthDocument52 pagesBacterial Meningitis Causes, Symptoms, and Diagnosis in Children Over 1 MonthTabada NickyNo ratings yet
- Prostate cancer differential diagnosis and key considerationsDocument4 pagesProstate cancer differential diagnosis and key considerationsRobert StolnicuNo ratings yet
- Diab 2013 JBack Musculoskel RehabilDocument8 pagesDiab 2013 JBack Musculoskel RehabilVineetha Victor GonsalvezNo ratings yet
- Villanueva 2016Document4 pagesVillanueva 2016OleOhhNo ratings yet
- Medicine CNS-ENDODocument11 pagesMedicine CNS-ENDOmrcopy xeroxNo ratings yet
- Recent Updates On Nanomedicine Based Products: Current Sce-Nario and Future OpportunitiesDocument13 pagesRecent Updates On Nanomedicine Based Products: Current Sce-Nario and Future OpportunitiesvijuNo ratings yet
- Slovenia's 25-year journey to help blood cancer patientsDocument40 pagesSlovenia's 25-year journey to help blood cancer patientsKlemen JamnikNo ratings yet
- ACUSON Antares Premium Edition BrochureDocument12 pagesACUSON Antares Premium Edition BrochureRanieh Al-Khatib100% (1)
- Lesson 1 - Matching HeadingDocument17 pagesLesson 1 - Matching HeadingHà ĐàoNo ratings yet
- Physical Health and Mental HealthDocument2 pagesPhysical Health and Mental HealthLuise MauieNo ratings yet
- Cigna Medical Coverage Policy For Sleep Testing ServicesDocument29 pagesCigna Medical Coverage Policy For Sleep Testing ServicesPhạm Văn HiệpNo ratings yet
- TSO Employee Details ListDocument107 pagesTSO Employee Details ListSanjan GhimireNo ratings yet
- Risk For Injury Related To Lack of KnowledgeDocument5 pagesRisk For Injury Related To Lack of KnowledgePaolo UyNo ratings yet
- Fetal DistressDocument49 pagesFetal DistressLenny SucalditoNo ratings yet
- L5 - Nature of Clinical Lab - PMLS1Document98 pagesL5 - Nature of Clinical Lab - PMLS1John Daniel AriasNo ratings yet
- What Are Water-Related Diseases? Water-Related Diseases and Their Control - Options For IntegrationDocument23 pagesWhat Are Water-Related Diseases? Water-Related Diseases and Their Control - Options For IntegrationBilal MemonNo ratings yet
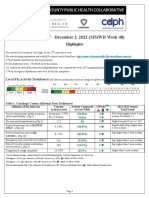
- 2022-23 Flu Surveillance Report - Week 48Document5 pages2022-23 Flu Surveillance Report - Week 48WKYC.comNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaUlfa RoisNo ratings yet
- Kibreet With ImagesDocument260 pagesKibreet With Imagesعباس عبداللهNo ratings yet
- Dashe 2013Document5 pagesDashe 2013Nữ Vương Nguyễn TrầnNo ratings yet
- Meda QantasDocument12 pagesMeda QantasAviasiNo ratings yet
- Historical SupplyDocument5 pagesHistorical Supplylara torricoNo ratings yet