You might also like
- Hazardous Substances and Human Health: Exposure, Impact and External Cost Assessment at the European ScaleFrom EverandHazardous Substances and Human Health: Exposure, Impact and External Cost Assessment at the European ScaleNo ratings yet
- Poster Ispe PDFDocument1 pagePoster Ispe PDFHadiantoNo ratings yet
- WHO IVB 14.07 EngDocument14 pagesWHO IVB 14.07 EnggineNo ratings yet
- Active Pharmaceutical Ingredients - Development, Manufacturing, and Regulation, Second Edition (Drugs and The Pharmaceutical Sciences) - 9781439803363 - Medicine & Health Science Books @Document13 pagesActive Pharmaceutical Ingredients - Development, Manufacturing, and Regulation, Second Edition (Drugs and The Pharmaceutical Sciences) - 9781439803363 - Medicine & Health Science Books @Marwa Ahmed100% (1)
- GMP For Facility Design References April06Document17 pagesGMP For Facility Design References April06madhubiochemNo ratings yet
- Animal Cell CultureDocument74 pagesAnimal Cell CultureMarcelo Andrés Ortiz BentoNo ratings yet
- Leseprobe FundamentalsDocument14 pagesLeseprobe FundamentalsDinesh SenathipathiNo ratings yet
- Premises As Per GMPDocument15 pagesPremises As Per GMPdivvelaNo ratings yet
- USFDA Pharmaceutical GuidelinesDocument5 pagesUSFDA Pharmaceutical GuidelinesemranNo ratings yet
- TKS 4155 Perancangan Pabrik: General Site ConsiderationsDocument35 pagesTKS 4155 Perancangan Pabrik: General Site ConsiderationsDavid BonjolNo ratings yet
- Vial washing for parenteral drugsDocument2 pagesVial washing for parenteral drugsAnas Abandeh100% (1)
- c1079 USP36 PDFDocument8 pagesc1079 USP36 PDFHassan HoudoudNo ratings yet
- A Final Floor Show For Bugs (Sandle)Document4 pagesA Final Floor Show For Bugs (Sandle)Tim Sandle100% (1)
- GMP Requirements for Ophthalmic Preparations SeminarDocument57 pagesGMP Requirements for Ophthalmic Preparations Seminarvkguptajss100% (1)
- Aseptic Process TechnologyDocument19 pagesAseptic Process TechnologyHimanshu ShahuNo ratings yet
- Basic Principles of GMP: GMP For Sterile Pharmaceutical ProductsDocument19 pagesBasic Principles of GMP: GMP For Sterile Pharmaceutical Productsabhijit_gothoskar6039No ratings yet
- Process Validation From An FDA Perspective - Part 2Document4 pagesProcess Validation From An FDA Perspective - Part 2Darren Tan100% (1)
- Maintenance QualificationDocument5 pagesMaintenance QualificationqlfangNo ratings yet
- ADC Skan Occupational SafetyDocument6 pagesADC Skan Occupational SafetyjmittalNo ratings yet
- Impact of Cross ContaminationDocument8 pagesImpact of Cross ContaminationYousifNo ratings yet
- InTech-Glp Good Laboratory PracticeDocument24 pagesInTech-Glp Good Laboratory PracticeTiwi100% (1)
- Cleaning Validation for Developmental, Stability and Clinical LotsDocument7 pagesCleaning Validation for Developmental, Stability and Clinical Lotszer-otakuNo ratings yet
- Bioburden USP PDFDocument4 pagesBioburden USP PDFKatyaSNNo ratings yet
- HAZOP Analysis Training GuideDocument7 pagesHAZOP Analysis Training GuideismailayarNo ratings yet
- Bioproc PDFDocument6 pagesBioproc PDFSrijit KhanNo ratings yet
- Pre-job Safety Briefing RequirementsDocument5 pagesPre-job Safety Briefing Requirementsliveconnectionz2820% (1)
- Quality by Design For Biotechnology Products-Part 2 - Process Development ForumDocument7 pagesQuality by Design For Biotechnology Products-Part 2 - Process Development ForumGyro9No ratings yet
- Apple Dylan Extensions and Framework ReferenceDocument714 pagesApple Dylan Extensions and Framework Referencepablo_marxNo ratings yet
- Lotus: Red Pharmtech Private LimitedDocument52 pagesLotus: Red Pharmtech Private LimitedprakashNo ratings yet
- ObjectionableDocument9 pagesObjectionabledmtalbhogeNo ratings yet
- Approaching Risk Assessment: Tools and MethodsDocument23 pagesApproaching Risk Assessment: Tools and MethodsTim Sandle100% (1)
- Testing Compressed Air Lines For Microbiological ContaminationDocument8 pagesTesting Compressed Air Lines For Microbiological Contaminationmuzammil21_adNo ratings yet
- Clean RoomDocument16 pagesClean RoomApoloTrevinoNo ratings yet
- Hazard and Risk Management - Sarika MamDocument24 pagesHazard and Risk Management - Sarika MamSharon DsouzaNo ratings yet
- What Is Good Engineering PracticeDocument4 pagesWhat Is Good Engineering PracticesarifinNo ratings yet
- Inherent Safety Design PrinciplesDocument19 pagesInherent Safety Design PrinciplesAbdurrahman OsailanNo ratings yet
- Application of PAT in Freeze-Drying of BiopharmaceuticalsDocument20 pagesApplication of PAT in Freeze-Drying of BiopharmaceuticalsKoushik PonnuruNo ratings yet
- Contamination ControlDocument5 pagesContamination ControlPadmanabhan DhanasekaranNo ratings yet
- 23635.1.5. Application of The F0 Concept To Steam Sterilisation of Aqueou - PDFDocument1 page23635.1.5. Application of The F0 Concept To Steam Sterilisation of Aqueou - PDFlilaNo ratings yet
- Research PaperDocument8 pagesResearch PaperBharat ParasharNo ratings yet
- Cohort of Concern Components and Analytical ChallengesDocument4 pagesCohort of Concern Components and Analytical ChallengeswoodsjaNo ratings yet
- Cross ContaminationDocument47 pagesCross ContaminationAKKAD PHARMANo ratings yet
- AIHce Pharma Forum Quality Risk-MaPP Implications - EditedDocument28 pagesAIHce Pharma Forum Quality Risk-MaPP Implications - EditedipliprensNo ratings yet
- Pharmaceutical Regulatory InspectionsDocument2 pagesPharmaceutical Regulatory InspectionsTim Sandle0% (1)
- FDA Warning Letter For Inadequate Batch Record ReviewDocument1 pageFDA Warning Letter For Inadequate Batch Record ReviewMina Maher MikhailNo ratings yet
- Aseptic ProcessingDocument13 pagesAseptic Processingnsk79in@gmail.comNo ratings yet
- Pharmaceutical excipients where do we beginDocument5 pagesPharmaceutical excipients where do we beginmads56091No ratings yet
- BPOG's ProtocolDocument11 pagesBPOG's ProtocolRadha Krishna B VNo ratings yet
- Introduction To ToxicologyDocument111 pagesIntroduction To ToxicologyaziskfNo ratings yet
- Strategic and Project ManagementDocument10 pagesStrategic and Project ManagementsurapolNo ratings yet
- Bioburden Recovery Method Using Swabbing TechniqueDocument8 pagesBioburden Recovery Method Using Swabbing TechniquePiruzi MaghlakelidzeNo ratings yet
- Veena SeminarDocument41 pagesVeena SeminarVeena PatilNo ratings yet
- GMP PartiiDocument76 pagesGMP PartiiRoger ManzanarezNo ratings yet
- Phuong - DryheatDocument5 pagesPhuong - DryheatqhpuongNo ratings yet
- Environmental Monitoring Risk AssessmentDocument22 pagesEnvironmental Monitoring Risk AssessmentMarcelo CarvalhoNo ratings yet
- QBD EMEA PPTDocument21 pagesQBD EMEA PPTElizabethValverde100% (1)
- Techniques for Downstream process for Biologic Drugs and VaccinesFrom EverandTechniques for Downstream process for Biologic Drugs and VaccinesNo ratings yet
- Biocontamination Control for Pharmaceuticals and HealthcareFrom EverandBiocontamination Control for Pharmaceuticals and HealthcareRating: 5 out of 5 stars5/5 (1)
- Proposal For SIMOPS VerificationDocument1 pageProposal For SIMOPS VerificationborrowmanaNo ratings yet
- Method of SupportDocument1 pageMethod of SupportborrowmanaNo ratings yet
- HAZOP and HAZID RecordDocument2 pagesHAZOP and HAZID RecordborrowmanaNo ratings yet
- Modified LOPA ProcedureDocument2 pagesModified LOPA ProcedureborrowmanaNo ratings yet
- HAZOP and HAZID RecordDocument2 pagesHAZOP and HAZID RecordborrowmanaNo ratings yet
- LOPA ProcedureDocument1 pageLOPA ProcedureborrowmanaNo ratings yet
- Environmental Consultant Scope of Work - FinalDocument10 pagesEnvironmental Consultant Scope of Work - FinalborrowmanaNo ratings yet
- SeaLion Due Diligence Report On Health and SafetyDocument29 pagesSeaLion Due Diligence Report On Health and SafetyborrowmanaNo ratings yet
- HAZID WorksheetDocument1 pageHAZID WorksheetborrowmanaNo ratings yet
- Case Study - Oil PlatformDocument5 pagesCase Study - Oil PlatformborrowmanaNo ratings yet
- Appendix II - Scope of ServicesDocument3 pagesAppendix II - Scope of ServicesborrowmanaNo ratings yet
- Hazop Study Action Response SheetDocument5 pagesHazop Study Action Response SheetborrowmanaNo ratings yet
- IEC Hazardous Locations Video Compares API/NEC and IEC ApproachesDocument2 pagesIEC Hazardous Locations Video Compares API/NEC and IEC ApproachesborrowmanaNo ratings yet
- SLR CONSULTING LIMITED Sub-Consultant's Agreement V3.1Document20 pagesSLR CONSULTING LIMITED Sub-Consultant's Agreement V3.1borrowmanaNo ratings yet
- Hazardous Area Classification: Codes of Practice and StandardsDocument13 pagesHazardous Area Classification: Codes of Practice and StandardsborrowmanaNo ratings yet
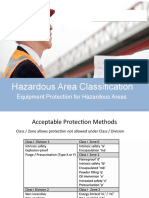
- Hazardous Area Classification: Equipment Protection For Hazardous AreasDocument22 pagesHazardous Area Classification: Equipment Protection For Hazardous AreasborrowmanaNo ratings yet
- Hazardous Area Classification Course OutlineDocument23 pagesHazardous Area Classification Course OutlineborrowmanaNo ratings yet
- ATEX NotesDocument9 pagesATEX NotesborrowmanaNo ratings yet
- Area ClassificationDocument28 pagesArea ClassificationborrowmanaNo ratings yet
- Hazardous Area Classification: Dusts and MistsDocument15 pagesHazardous Area Classification: Dusts and MistsborrowmanaNo ratings yet
- Using HAC For Gas Detector LayoutsDocument8 pagesUsing HAC For Gas Detector LayoutsborrowmanaNo ratings yet
- Hazardous Area Classification: Equipment Protection For Hazardous AreasDocument22 pagesHazardous Area Classification: Equipment Protection For Hazardous AreasborrowmanaNo ratings yet
- Hazardous Area Classification: Certification and Equipment MarkingDocument4 pagesHazardous Area Classification: Certification and Equipment MarkingborrowmanaNo ratings yet
- Hazardous Area Classification: Certification and Equipment MarkingDocument4 pagesHazardous Area Classification: Certification and Equipment MarkingborrowmanaNo ratings yet
- Hazardous Area Classification: Codes of Practice and StandardsDocument13 pagesHazardous Area Classification: Codes of Practice and StandardsborrowmanaNo ratings yet
- Hazardous Area Classification Course OutlineDocument23 pagesHazardous Area Classification Course OutlineborrowmanaNo ratings yet
- Area ClassificationDocument28 pagesArea ClassificationborrowmanaNo ratings yet
- Case Study - Oil PlatformDocument5 pagesCase Study - Oil PlatformborrowmanaNo ratings yet
- Using HAC For Gas Detector LayoutsDocument8 pagesUsing HAC For Gas Detector LayoutsborrowmanaNo ratings yet
- Hazardous Area Classification: Dusts and MistsDocument15 pagesHazardous Area Classification: Dusts and MistsborrowmanaNo ratings yet
- U.S. Pipelines & Logistics Health, Safety, Security Environmental (HSSE) PolicyDocument1 pageU.S. Pipelines & Logistics Health, Safety, Security Environmental (HSSE) PolicyAmiibahNo ratings yet
- Better Forecasting For Large Capital ProjectsDocument7 pagesBetter Forecasting For Large Capital ProjectsJMNo ratings yet
- PETRONAS Canada 2020 04 Policy HSSEDocument11 pagesPETRONAS Canada 2020 04 Policy HSSELearning的生活No ratings yet
- Effects of Globalization On Indian Insurance SectorDocument21 pagesEffects of Globalization On Indian Insurance SectorArindam DeyNo ratings yet
- Importance of Governance, Risk, and Compliance Principles: ChaptertwoDocument10 pagesImportance of Governance, Risk, and Compliance Principles: ChaptertwoYuris ZegaNo ratings yet
- RMTH Chapter OneDocument42 pagesRMTH Chapter Onesosina eseyewNo ratings yet
- The Story of Statistics in Geotechnical EngineeringDocument24 pagesThe Story of Statistics in Geotechnical EngineeringfakeNo ratings yet
- NucleonDocument12 pagesNucleonPriya Singh100% (3)
- Innovative ManagementDocument10 pagesInnovative ManagementainaNo ratings yet
- Acute Support Allied Health Clinical PrioritisationDocument4 pagesAcute Support Allied Health Clinical Prioritisationece142No ratings yet
- SEC Complaint V Vale SADocument76 pagesSEC Complaint V Vale SATim MooreNo ratings yet
- Investigations ManualDocument99 pagesInvestigations Manualbocy me100% (1)
- COSO I e IIDocument9 pagesCOSO I e IIcarakholNo ratings yet
- Reach Out Educator Manual PDFDocument136 pagesReach Out Educator Manual PDFSze01No ratings yet
- Trulieve IR Deck Nov 2019 - NewDocument19 pagesTrulieve IR Deck Nov 2019 - NewstonerhinoNo ratings yet
- API 141 Syllabus Fall 2023 - SEPT2023Document20 pagesAPI 141 Syllabus Fall 2023 - SEPT2023ElvinP.AliyevNo ratings yet
- Valley Silts DSR Public Review 20190726Document130 pagesValley Silts DSR Public Review 20190726Greefield JasonNo ratings yet
- S-001 (Technical Safety)Document72 pagesS-001 (Technical Safety)syamsudin2006No ratings yet
- LVA-i 3 User GuideDocument36 pagesLVA-i 3 User GuideGabriel ArriolaNo ratings yet
- Commodities in 2023 V4Document8 pagesCommodities in 2023 V4Luiggi Andre Castro RumicheNo ratings yet
- Introtociscosafe 2023 PDFDocument50 pagesIntrotociscosafe 2023 PDFMichael O'ConnellNo ratings yet
- Weebly ArticleDocument22 pagesWeebly Articleapi-315662328No ratings yet
- SOP Ethics Committee IHBASDocument23 pagesSOP Ethics Committee IHBASlessysajeevNo ratings yet
- CPG RESTRAIN GuidelinesDocument8 pagesCPG RESTRAIN GuidelinesaartiNo ratings yet
- Design and Selection of TrolleysDocument8 pagesDesign and Selection of TrolleysBawa SandhuNo ratings yet
- 4 Things To ConsiderDocument11 pages4 Things To ConsiderferengoNo ratings yet
- IT8075 UNIT 1 Activities - MethodologiesDocument39 pagesIT8075 UNIT 1 Activities - MethodologiesS RNo ratings yet
- When AI Meets Information Privacy The Adversarial Role of AI in Data Sharing ScenarioDocument19 pagesWhen AI Meets Information Privacy The Adversarial Role of AI in Data Sharing ScenarioNGuyen thi Kim TuyenNo ratings yet
- 3q21 Earnings ReleaseDocument5 pages3q21 Earnings ReleaseBruno EnriqueNo ratings yet
- Case Study: RBI and Its Application To Inspection of DHTU Flare Knockout DrumsDocument25 pagesCase Study: RBI and Its Application To Inspection of DHTU Flare Knockout Drumsjasminnee100% (1)