You might also like
- Bacaan PPT RebleedingDocument61 pagesBacaan PPT RebleedingseliNo ratings yet
- 701 2022 Article 5445Document9 pages701 2022 Article 5445PeyepeyeNo ratings yet
- Approach To A Patient With Gastric VaricesDocument19 pagesApproach To A Patient With Gastric VaricesGavi Siddanagowda PatilNo ratings yet
- Stenosis AV Fistulas: Obobku Sayang SemangaaaatttttDocument17 pagesStenosis AV Fistulas: Obobku Sayang SemangaaaatttttraissaNo ratings yet
- Catheter Ablation of Intramural Outflow Tract Premature Ventricular Complexes - A Multicentre StudyDocument9 pagesCatheter Ablation of Intramural Outflow Tract Premature Ventricular Complexes - A Multicentre Studyahmed mostafaNo ratings yet
- Transplantation 2Document55 pagesTransplantation 2Shahansha Sharan DhammatiNo ratings yet
- Vascular Graft Infection: An: Presented By: Nader Saad - PGY2 Vascular SurgeryDocument42 pagesVascular Graft Infection: An: Presented By: Nader Saad - PGY2 Vascular SurgeryNader SaadNo ratings yet
- Khairy 2017Document7 pagesKhairy 2017Beby Dwi Lestari BajryNo ratings yet
- Cardiac Catheterization Complications Modulo 1Document32 pagesCardiac Catheterization Complications Modulo 1Isabel PauloNo ratings yet
- Postoperative Complication of Colorectal SurgeryDocument29 pagesPostoperative Complication of Colorectal SurgeryPeter ChenNo ratings yet
- Budd Chiari SyndromeDocument37 pagesBudd Chiari SyndromeNader SaadNo ratings yet
- Multimodal Tretment of Intracranial Aneurysm: A. Chiriac, I. Poeata, J. Baldauf, H.W. SchroederDocument10 pagesMultimodal Tretment of Intracranial Aneurysm: A. Chiriac, I. Poeata, J. Baldauf, H.W. SchroederApryana Damayanti ARNo ratings yet
- Tavi 13Document8 pagesTavi 13a f indra pratamaNo ratings yet
- Vascular Interventional RadiologyDocument1 pageVascular Interventional RadiologywhitecoatNo ratings yet
- Brant and Helms Ch. 25 Interventional RadiologyDocument72 pagesBrant and Helms Ch. 25 Interventional RadiologyjastevensonNo ratings yet
- Indications, Contraindications, Complications & Adjuvant Pharmacology-3Document24 pagesIndications, Contraindications, Complications & Adjuvant Pharmacology-3Fiza MushtaqNo ratings yet
- Esophageal and Gastric VaricesDocument15 pagesEsophageal and Gastric VaricesDumbo D' CatNo ratings yet
- Complications of Percutaneous Coronary Interventions and ManagementDocument10 pagesComplications of Percutaneous Coronary Interventions and ManagementshyluckmayddpNo ratings yet
- Endoscopicmanagementof Portalhypertension-Related Bleeding: Andrew Nett,, Kenneth F. BinmoellerDocument17 pagesEndoscopicmanagementof Portalhypertension-Related Bleeding: Andrew Nett,, Kenneth F. BinmoellerAlonso CayaniNo ratings yet
- Novel Thrombus Removal DeviceDocument2 pagesNovel Thrombus Removal Device钟斌No ratings yet
- Endovascular Therapy For Central Venous ThrombosisDocument5 pagesEndovascular Therapy For Central Venous ThrombosissukiyantoNo ratings yet
- Percutaneous Coronary InterventionDocument20 pagesPercutaneous Coronary InterventionDeepika PatelNo ratings yet
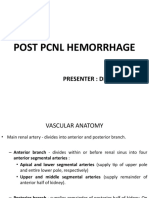
- Post PCNL Hemorrhage: Presenter: DR Sumit KabraDocument30 pagesPost PCNL Hemorrhage: Presenter: DR Sumit KabraGaurav GuptaNo ratings yet
- Varicose Vein Treatment Tips and Trick - Ablation or GlueDocument30 pagesVaricose Vein Treatment Tips and Trick - Ablation or GlueNata NakamuraNo ratings yet
- 11 Caring For Patients Post PCI Emil 2019Document3 pages11 Caring For Patients Post PCI Emil 2019ameliajamirusNo ratings yet
- Esophageal Varices SclerotherapyDocument15 pagesEsophageal Varices Sclerotherapynana wandhanaNo ratings yet
- Pci 1Document24 pagesPci 1shejila c hNo ratings yet
- Anaesthesia For Endovascular Surgery (Tevar and EvarDocument18 pagesAnaesthesia For Endovascular Surgery (Tevar and EvaranaeshklNo ratings yet
- RadiologyDocument46 pagesRadiologyitho23100% (1)
- Angioplasty and Vascular StentingDocument8 pagesAngioplasty and Vascular Stentingrajnishpathak648No ratings yet
- Advances in Tunneled CVCDsDocument12 pagesAdvances in Tunneled CVCDsroykelumendekNo ratings yet
- Vein - 2009 Sir - Ivcf ReviewDocument9 pagesVein - 2009 Sir - Ivcf Reviewjohn_smith_532No ratings yet
- Adenosine-Induced Transient Asystole: Gavin W. Britz, M.D., M.P.HDocument4 pagesAdenosine-Induced Transient Asystole: Gavin W. Britz, M.D., M.P.HAnkitaNo ratings yet
- Pseudoanuerysms Made EasyDocument15 pagesPseudoanuerysms Made EasyFooffscribdNo ratings yet
- Varicocele Is A Clinical Diagnosis Established by Physical Exam Performed inDocument4 pagesVaricocele Is A Clinical Diagnosis Established by Physical Exam Performed inSi Aniel TohNo ratings yet
- Management of Lower GI BleedDocument48 pagesManagement of Lower GI Bleednameless111100No ratings yet
- Overview of FistulasDocument39 pagesOverview of FistulasWade JacksonNo ratings yet
- Aortic Aneurysm: DR Rahul CDocument79 pagesAortic Aneurysm: DR Rahul CIrwan Meidi LubisNo ratings yet
- Thoracic and Abdominal TraumaDocument76 pagesThoracic and Abdominal Traumajhk0428100% (1)
- Abdominal Aortic Aneurysm 1Document45 pagesAbdominal Aortic Aneurysm 1hemanarasimha gandikotaNo ratings yet
- Local Vascular ComplicationsDocument3 pagesLocal Vascular ComplicationsKaterina FusaNo ratings yet
- Subarachnoid Hemorrhage: Hania El Jarkass, MD Neurology MGHDocument30 pagesSubarachnoid Hemorrhage: Hania El Jarkass, MD Neurology MGHamal najaNo ratings yet
- HemodialysisDocument11 pagesHemodialysisjuan_sioNo ratings yet
- Vascular AccessDocument51 pagesVascular Accesssantosh subediNo ratings yet
- S0090429521002594Document7 pagesS0090429521002594Mounia MarsouNo ratings yet
- RTC Spleen InjuryDocument51 pagesRTC Spleen InjuryKenny FathurNo ratings yet
- Lower Gi Bleed 4611Document23 pagesLower Gi Bleed 4611Mien BuntaraNo ratings yet
- Journaloftheamericancollegeofcardiology, Vol 67, No 16, Suppls, 2016Document2 pagesJournaloftheamericancollegeofcardiology, Vol 67, No 16, Suppls, 2016Priscilla Rachel MeganathanNo ratings yet
- Varicose Veins of The Lower Extremities Treatment ForDocument17 pagesVaricose Veins of The Lower Extremities Treatment ForsalinasjulioNo ratings yet
- Nasser Et Al. - 2013 - Use of Transoesophageal Echocardiography in Endovascular Stenting For Superior Vena Cava SyndromeDocument3 pagesNasser Et Al. - 2013 - Use of Transoesophageal Echocardiography in Endovascular Stenting For Superior Vena Cava SyndromeflashjetNo ratings yet
- Tavi 18Document3 pagesTavi 18a f indra pratamaNo ratings yet
- Abdominal Aortic Aneurysm 1Document44 pagesAbdominal Aortic Aneurysm 1Kendy Rizky Hadyan100% (1)
- IVUS OCT Guidance of IVL 2020 Mateissi, Mamas Et Al.Document7 pagesIVUS OCT Guidance of IVL 2020 Mateissi, Mamas Et Al.PraveenVeeraNo ratings yet
- Technology Assessment Status Evaluation Endoscopic Band Ligation of VaricesDocument3 pagesTechnology Assessment Status Evaluation Endoscopic Band Ligation of VaricesElmer PalaciosNo ratings yet
- 16 Lawrence Should Subclavian Vein Thrombosis Always Be Treated With Rib ResectionDocument6 pages16 Lawrence Should Subclavian Vein Thrombosis Always Be Treated With Rib ResectionMiroslav TrpkovicNo ratings yet
- Catheter-Related Thrombosis - Approach 2016Document8 pagesCatheter-Related Thrombosis - Approach 2016Le ThyNo ratings yet
- TURBT FinalDocument52 pagesTURBT FinalMuhammad RafiNo ratings yet
- Percutaneous Nephrostomy: Last Updated: January 3, 2003Document5 pagesPercutaneous Nephrostomy: Last Updated: January 3, 2003Alicia EncinasNo ratings yet
- Management of Lower GI BleedDocument48 pagesManagement of Lower GI BleedMegat Mohd Azman AdzmiNo ratings yet
- Aortic RegurgitationFrom EverandAortic RegurgitationJan VojacekNo ratings yet
- Slide Dr. RifqiDocument42 pagesSlide Dr. RifqiAndrew E P SunardiNo ratings yet
- ECG ReadingDocument10 pagesECG ReadingAndrew E P SunardiNo ratings yet
- Diuretic Resistance in Heart Failure.99668 PDFDocument44 pagesDiuretic Resistance in Heart Failure.99668 PDFAndrew E P SunardiNo ratings yet
- ECG ReadingDocument10 pagesECG ReadingAndrew E P SunardiNo ratings yet
- Diuretic Resistance in Heart Failure.99668 PDFDocument44 pagesDiuretic Resistance in Heart Failure.99668 PDFAndrew E P SunardiNo ratings yet
- Acute Non Cardiac Failure in Cardiogenic Shock PDFDocument11 pagesAcute Non Cardiac Failure in Cardiogenic Shock PDFAndrew E P SunardiNo ratings yet
- Acute Non Cardiac Failure in Cardiogenic Shock PDFDocument11 pagesAcute Non Cardiac Failure in Cardiogenic Shock PDFAndrew E P SunardiNo ratings yet
- Effects of Sex On Coronary Microvascular Dysfunction and Cardiac OutcomesDocument10 pagesEffects of Sex On Coronary Microvascular Dysfunction and Cardiac OutcomesAndrew E P SunardiNo ratings yet
- Overview of Basic Mechanisms of Cardiac ArrhythmiaDocument23 pagesOverview of Basic Mechanisms of Cardiac ArrhythmiaKevin Mora BañosNo ratings yet
- Overview of Basic Mechanisms of Cardiac ArrhythmiaDocument23 pagesOverview of Basic Mechanisms of Cardiac ArrhythmiaKevin Mora BañosNo ratings yet
- Peters 2014Document10 pagesPeters 2014Andrew E P SunardiNo ratings yet
- Charytan 2017Document9 pagesCharytan 2017Andrew E P SunardiNo ratings yet
- Coronary Microvascular Rarefaction and Myocardial Fibrosis in Heart Failure With Preserved Ejection FractionDocument10 pagesCoronary Microvascular Rarefaction and Myocardial Fibrosis in Heart Failure With Preserved Ejection FractionAndrew E P SunardiNo ratings yet
- Atherosclerotic Heart DiseaseDocument9 pagesAtherosclerotic Heart DiseaseWynoaj LucaNo ratings yet
- Good Thesis Statement For Heart DiseaseDocument5 pagesGood Thesis Statement For Heart Diseasemarilynmarieboston100% (2)
- Fungal Mycotoxin ConnectionDocument2 pagesFungal Mycotoxin Connectionapi-3695725100% (1)
- Meet The Profesor 2021Document398 pagesMeet The Profesor 2021Raúl AssadNo ratings yet
- BIOLOGY INVESTIGATORY PROJECT - Cardiovascular Diseases - Coronary Artery Disease PDFDocument50 pagesBIOLOGY INVESTIGATORY PROJECT - Cardiovascular Diseases - Coronary Artery Disease PDFlskumar100% (1)
- An Approach To Acute Coronary Syndrome (ACS) : DR Harihar KhanalDocument60 pagesAn Approach To Acute Coronary Syndrome (ACS) : DR Harihar KhanalDr Harihar KhanalNo ratings yet
- Biology Notes Chpter 10Document8 pagesBiology Notes Chpter 10Wan HasliraNo ratings yet
- Hipertriglicerida Pada AnakDocument44 pagesHipertriglicerida Pada AnakannisanangNo ratings yet
- Tumors 0F CNS-1Document25 pagesTumors 0F CNS-1Mo HamoudNo ratings yet
- Free Radicals and Reactive Oxygen SpeciesDocument17 pagesFree Radicals and Reactive Oxygen SpeciesSyncOrSwim100% (2)
- Cerebrovascular AccidentDocument30 pagesCerebrovascular AccidentRichard Charles UmlasNo ratings yet
- Ellison - Hidden Truth About Cholesterol-Lowering Drugs (2006) PDFDocument42 pagesEllison - Hidden Truth About Cholesterol-Lowering Drugs (2006) PDFridwansurono100% (2)
- 11 CholesterolDocument48 pages11 CholesterolClaudiaNathaliaNo ratings yet
- 040-444 ACSM Registered Clinical Exercise PhysiologistDocument101 pages040-444 ACSM Registered Clinical Exercise PhysiologistKamran MusaNo ratings yet
- Heart MattersDocument39 pagesHeart MattersGerry OshNo ratings yet
- Coronary Microvascular Disease Pathogenic Mechanisms and Therapeutic OptionsDocument17 pagesCoronary Microvascular Disease Pathogenic Mechanisms and Therapeutic OptionsZuleynny TellesNo ratings yet
- 4 - Patophysiology of Cardiovascular Disease PPDocument126 pages4 - Patophysiology of Cardiovascular Disease PPFirdaws FaxirNo ratings yet
- Essential of Special Patholog by DR Zair Hassan: December 2015Document271 pagesEssential of Special Patholog by DR Zair Hassan: December 2015pdf pediatriNo ratings yet
- Zuac 123Document11 pagesZuac 123Nelson Da VegaNo ratings yet
- Appendix B-Acceptable AcronymsDocument11 pagesAppendix B-Acceptable AcronymsKimberly SolisNo ratings yet
- Textbook of Cardiovascular MedicineDocument3,088 pagesTextbook of Cardiovascular MedicineAndreea Alina Tanase100% (4)
- Senka Mesihovic-Dinarevic Lutvo Sporisevic, Chapter IIDocument11 pagesSenka Mesihovic-Dinarevic Lutvo Sporisevic, Chapter IIvaria5No ratings yet
- Lesson Plan Grade 7Document15 pagesLesson Plan Grade 7RoseMayHagnaNo ratings yet
- KIF6 Genotyping For Predicting Cardiovascular Risk And/or Effectiveness of Statin TherapyDocument7 pagesKIF6 Genotyping For Predicting Cardiovascular Risk And/or Effectiveness of Statin TherapyDavid BriggsNo ratings yet
- Pathophysiology QBDocument5 pagesPathophysiology QBVimlesh PalNo ratings yet
- Atherosclerotic Cardiovascular DiseaseDocument68 pagesAtherosclerotic Cardiovascular DiseaseMarisa Adytia Adha100% (1)
- Circulatory SystemsDocument4 pagesCirculatory SystemsMarielle GodoyNo ratings yet
- A Bornstein, MD, FACC Assistant Professor of Public Health Weill Cornell Medical CollegeDocument50 pagesA Bornstein, MD, FACC Assistant Professor of Public Health Weill Cornell Medical CollegeSyed ImranNo ratings yet
- Hypertension Clinical Study PDFDocument42 pagesHypertension Clinical Study PDFsertti23No ratings yet
- Guidelines Peripheral AD FTDocument56 pagesGuidelines Peripheral AD FTVisoiu Ioan-LucianNo ratings yet