You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Ferguson - Preparatory Exercises in Score ReadingDocument122 pagesFerguson - Preparatory Exercises in Score ReadingAndrea Roja Rojnić100% (14)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Subliminal Bundle - BenefitsDocument21 pagesSubliminal Bundle - BenefitsVicky CallenreeseNo ratings yet
- MODAL VERBS Must:have To:should:ought To ExercisesDocument3 pagesMODAL VERBS Must:have To:should:ought To ExercisesQuỳnh Anh LêNo ratings yet
- Atenolol Oral Suspension 2mg/mLDocument1 pageAtenolol Oral Suspension 2mg/mLChemistixNo ratings yet
- A Paediatric Musculoskeletal Competence FrameworkDocument18 pagesA Paediatric Musculoskeletal Competence FrameworkPT Depart AMCHNo ratings yet
- National Mental Health ProgramDocument18 pagesNational Mental Health ProgramDIYA DINDANo ratings yet
- Group DR - Script - Allergic Rhinitis (Peanut Allergy) Health EducationDocument10 pagesGroup DR - Script - Allergic Rhinitis (Peanut Allergy) Health EducationKyra Bianca R. FamacionNo ratings yet
- Thesis On Motivational InterviewingDocument8 pagesThesis On Motivational Interviewingwendyfoxdesmoines100% (1)
- Finishing CarpentryDocument25 pagesFinishing CarpentryKevin Fernandez MendioroNo ratings yet
- Research MethodologyDocument4 pagesResearch MethodologySubrat RathNo ratings yet
- Developing The 21st-Century Leader - Global Trends in Leadership Challenges and Practices 2010 PDFDocument32 pagesDeveloping The 21st-Century Leader - Global Trends in Leadership Challenges and Practices 2010 PDFNashwa SaadNo ratings yet
- GP - Clinics 2020 07Document44 pagesGP - Clinics 2020 07Mustafa BapaiNo ratings yet
- Perio ProjectDocument26 pagesPerio Projectkhaled alahmadNo ratings yet
- Англійська моваDocument41 pagesАнглійська моваLê TùngNo ratings yet
- The NCLEX-RN Exam Study Guide Premium Edition - Proven Methods To Pass The NCLEX-RN Examination With Confidence (Belinelli, Rachel Media Group, Scientia) PDFDocument509 pagesThe NCLEX-RN Exam Study Guide Premium Edition - Proven Methods To Pass The NCLEX-RN Examination With Confidence (Belinelli, Rachel Media Group, Scientia) PDFColeen Yraola80% (5)
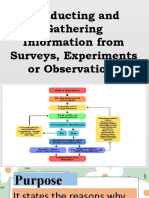
- Conducting and Gathering Information From Surveys, Experiments or ObservationsDocument53 pagesConducting and Gathering Information From Surveys, Experiments or ObservationsJannet Calma LansanganNo ratings yet
- GRP 7 Partograph BSN - 2DDocument13 pagesGRP 7 Partograph BSN - 2DCzarina Mae Quinones Tadeo0% (1)
- Non Dioxine Certificate-TemplateDocument1 pageNon Dioxine Certificate-Templateadnanbajwa141No ratings yet
- استراتيجيات التدريس لذوي الاعاقة السمعيةDocument13 pagesاستراتيجيات التدريس لذوي الاعاقة السمعيةmimimil0707No ratings yet
- AllopurinolDocument1 pageAllopurinolMelissa VilarNo ratings yet
- Article Trailer Script and Sources. ScriptDocument2 pagesArticle Trailer Script and Sources. ScriptEvol 9897No ratings yet
- Abuse RoP Checklist - 1 PDFDocument7 pagesAbuse RoP Checklist - 1 PDFArlene AngelesNo ratings yet
- Adult Health Nursing I LAB Syllabus 2020-2021Document195 pagesAdult Health Nursing I LAB Syllabus 2020-2021Hajer AlowaisiNo ratings yet
- 07 Handout 1 PerDevDocument1 page07 Handout 1 PerDevKing CjNo ratings yet
- Impact of Compensation and Benefits On Job SatisfactionDocument12 pagesImpact of Compensation and Benefits On Job SatisfactionDesita Anggra DewiNo ratings yet
- DLSMHSI SHS Faculty Manual 2019-2012 (Web)Document234 pagesDLSMHSI SHS Faculty Manual 2019-2012 (Web)Lorlie AbrogarNo ratings yet
- Nature of CounselingDocument6 pagesNature of CounselingNathalie ReyesNo ratings yet
- Prepared By: Lelibeth PobleteDocument56 pagesPrepared By: Lelibeth PobleteRheda DrawsNo ratings yet
- Anna Mogills Resume 4Document2 pagesAnna Mogills Resume 4api-454132902No ratings yet
- European Solidarity Corps Guide 2023 enDocument112 pagesEuropean Solidarity Corps Guide 2023 entanrigunverdi'accountNo ratings yet