You might also like
- 4 ImpactionDocument188 pages4 ImpactionD YasIr MussaNo ratings yet
- Bhanu Impaction Seminar FinalDocument138 pagesBhanu Impaction Seminar FinalBhanu PraseedhaNo ratings yet
- Cervical LesionsDocument135 pagesCervical Lesionsrasagna reddyNo ratings yet
- Wisdom Teeth: Fact or Myth ??: Dr. Ali Waqar Resident Fcps - Ii Orthodontics Ucmd Uol LahoreDocument20 pagesWisdom Teeth: Fact or Myth ??: Dr. Ali Waqar Resident Fcps - Ii Orthodontics Ucmd Uol LahoreIsaac NsengaNo ratings yet
- Etiology Local FactorsDocument41 pagesEtiology Local Factorskaran patelNo ratings yet
- IMPACTIONDocument127 pagesIMPACTIONAbhishek JhaNo ratings yet
- Lecture 2 Tooth Eruption and SheddingDocument35 pagesLecture 2 Tooth Eruption and SheddingAMIT GUPTANo ratings yet
- Management of Delayed Eruption of Perma-Nent Maxillary Incisor Associated With The Presence of Supernumerary Teeth: A Case ReportDocument5 pagesManagement of Delayed Eruption of Perma-Nent Maxillary Incisor Associated With The Presence of Supernumerary Teeth: A Case ReportFelianda ThaliaNo ratings yet
- Presentation2 Impaction (Online)Document91 pagesPresentation2 Impaction (Online)lola abualillNo ratings yet
- ImpactionDocument81 pagesImpactionShouvik Chowdhury50% (6)
- Seminar 7Document28 pagesSeminar 7Dan 04No ratings yet
- Shedding of TeethDocument23 pagesShedding of TeethsiddarthNo ratings yet
- Mandibular Third Molar Impactions NotesDocument18 pagesMandibular Third Molar Impactions NotesJoseph John K Pothanikat100% (1)
- Teeth, Genes, and GenealogyDocument4 pagesTeeth, Genes, and GenealogyPablo BenitezNo ratings yet
- Delayed Tooth EmergenceDocument16 pagesDelayed Tooth EmergenceValeria CernegaNo ratings yet
- Isolated Dental Anomalies Class I Angle: Supernumerary Teeth AnodontiaDocument43 pagesIsolated Dental Anomalies Class I Angle: Supernumerary Teeth AnodontiaAdelina IacomiNo ratings yet
- Developmental Disorders of TeethDocument64 pagesDevelopmental Disorders of TeethPatterson MachariaNo ratings yet
- (1995) LUKACS, J. R. .Dental DeductionsDocument29 pages(1995) LUKACS, J. R. .Dental DeductionsÉrikaOrtsacNo ratings yet
- Supernumerary Lateral IncisorDocument2 pagesSupernumerary Lateral IncisorNatasa StojkovicNo ratings yet
- Open BiteDocument14 pagesOpen Biteفاطمة فالح ضايف مزعلNo ratings yet
- Etiology of Orthodontic ProblemsDocument85 pagesEtiology of Orthodontic ProblemsShahid Hameed0% (1)
- Development of Dentition WordDocument21 pagesDevelopment of Dentition Wordshubhangi_jain_10100% (1)
- Iagnosis and Treatment Planning For Complete Dentures: by Dr. Muhammad Afzal RegistrarDocument44 pagesIagnosis and Treatment Planning For Complete Dentures: by Dr. Muhammad Afzal Registrargeeta aryaNo ratings yet
- Tooth Ankylosis and Its Orthodontic ImplicationDocument5 pagesTooth Ankylosis and Its Orthodontic ImplicationagdroubiNo ratings yet
- Supernumerary and Congenitally Absent Teeth A Literature ReviewDocument6 pagesSupernumerary and Congenitally Absent Teeth A Literature Reviewea6z9033No ratings yet
- Sakeena Assad PresentationDocument93 pagesSakeena Assad Presentationjenny girlNo ratings yet
- Ectopic Tooth in The Anterior Wall of The Maxillary SinusDocument3 pagesEctopic Tooth in The Anterior Wall of The Maxillary Sinuspunct_org3256No ratings yet
- Stone Age Mans Dentition2 Ajo1954Document11 pagesStone Age Mans Dentition2 Ajo1954BeniyaNo ratings yet
- Multi-Lobed Mesiodens With A Palatal Talon Cusp - A Rare Case ReportDocument4 pagesMulti-Lobed Mesiodens With A Palatal Talon Cusp - A Rare Case ReportWira WinataNo ratings yet
- Dental CariesDocument209 pagesDental Cariesdrhiteshk75% (4)
- The Management of Palatally DisplacedDocument13 pagesThe Management of Palatally DisplacedFourthMolar.comNo ratings yet
- Dev DisordersDocument16 pagesDev DisordersPragatiNo ratings yet
- MonographTsvetanovPechalova EditedbyProfessorAngelBakardjievDocument82 pagesMonographTsvetanovPechalova EditedbyProfessorAngelBakardjievpratyusha vallamNo ratings yet
- AOT (Adenomatoid Odontogenic Tumor) : Pyogenic GranulomaDocument54 pagesAOT (Adenomatoid Odontogenic Tumor) : Pyogenic GranulomaSanNo ratings yet
- DistomolerDocument5 pagesDistomolerMukarram FaridiNo ratings yet
- Non-Syndromic Multiple Mesiodens: Two Case ReportsDocument3 pagesNon-Syndromic Multiple Mesiodens: Two Case ReportsWilliam YuwonoNo ratings yet
- Dental Erosion. Definition, Classification and LinksDocument5 pagesDental Erosion. Definition, Classification and LinksRusevNo ratings yet
- Aetiology of Malocclusion of The TeethDocument2 pagesAetiology of Malocclusion of The TeethBob Permana Simanungkalit100% (1)
- Detained and Semidedetatained Teeth.Document19 pagesDetained and Semidedetatained Teeth.Vikas BhattNo ratings yet
- Development of DentitionDocument79 pagesDevelopment of Dentitionswathi datrika100% (1)
- Nonsyndromic Delayed EruptionDocument3 pagesNonsyndromic Delayed EruptionRista LewiyonahNo ratings yet
- Impaction SDocument127 pagesImpaction SVaibhav Nagaraj75% (4)
- Cysts of The JawsDocument26 pagesCysts of The JawsPranay NeemaNo ratings yet
- Developmental Anomalies of TeethDocument97 pagesDevelopmental Anomalies of Teethtopuzoglualeyna5No ratings yet
- OriginalDocument10 pagesOriginalAmir IqbalNo ratings yet
- Odonto ExoticosDocument14 pagesOdonto ExoticosPedro FontaniveNo ratings yet
- Anthropology and Its Relation To Orthodontics - Part 2Document4 pagesAnthropology and Its Relation To Orthodontics - Part 2Saumya SinghNo ratings yet
- Histology and Physiology of The Dental Pulp: David H. Pashley, Richard E. Walton, and Harold C. SlavkinDocument39 pagesHistology and Physiology of The Dental Pulp: David H. Pashley, Richard E. Walton, and Harold C. SlavkinHeng SiekhongNo ratings yet
- Sajnani, 2015Document7 pagesSajnani, 2015Julio AbarzuaNo ratings yet
- Extracciones Seriadas 15Document8 pagesExtracciones Seriadas 15Mirita AliauNo ratings yet
- Non Carious Lesions and Their ManagementDocument47 pagesNon Carious Lesions and Their ManagementDrApplu Atrey50% (2)
- 8 Tooth Ankylosis Andits Orthodontic ImplicationDocument6 pages8 Tooth Ankylosis Andits Orthodontic ImplicationPretty HiaNo ratings yet
- Dental Caries FinalDocument40 pagesDental Caries FinalSimran KathuriaNo ratings yet
- Direct Factors Affecting The PeriodontiumDocument4 pagesDirect Factors Affecting The PeriodontiumHayley WelshNo ratings yet
- MesiodensDocument20 pagesMesiodenslaydee_melaNo ratings yet
- Bilaterally Impacted Mandibular Supernumerary Premolars Associated With Unusual Clinical ComplicationsDocument5 pagesBilaterally Impacted Mandibular Supernumerary Premolars Associated With Unusual Clinical ComplicationsAira Grace PadillaNo ratings yet
- Pulp and InjuryDocument13 pagesPulp and InjuryAfin Aslihatul UmmahNo ratings yet
- Regressive Alterations of TeethDocument71 pagesRegressive Alterations of TeethCreatingWisdom100% (1)
- Serial Extractions - A Review PDFDocument8 pagesSerial Extractions - A Review PDFJose CollazosNo ratings yet
- East Side ElevationDocument1 pageEast Side ElevationRichaNo ratings yet
- Centerline PlanDocument1 pageCenterline PlanRichaNo ratings yet
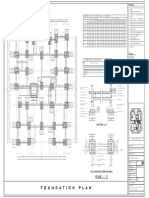
- Foundation PlanDocument1 pageFoundation PlanRichaNo ratings yet
- Key Plan: Detail Counter Detail at Window Cill and JambDocument1 pageKey Plan: Detail Counter Detail at Window Cill and JambRichaNo ratings yet
- Key Plan: Detail Counter Detail at Window Cill and JambDocument1 pageKey Plan: Detail Counter Detail at Window Cill and JambRichaNo ratings yet
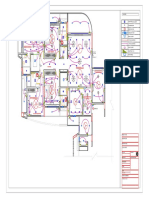
- Electrical LayoutDocument1 pageElectrical LayoutRichaNo ratings yet
- Key Plan: Detail at Window Sill and JambDocument1 pageKey Plan: Detail at Window Sill and JambRichaNo ratings yet
- Richa Sharma - 2018163T - Div B - Abcm - Assignments PDFDocument63 pagesRicha Sharma - 2018163T - Div B - Abcm - Assignments PDFRichaNo ratings yet
- Key Plan: Detail CounterDocument1 pageKey Plan: Detail CounterRichaNo ratings yet
- 9.00 M Internal Road 9.00 M Internal Road: Water BodyDocument1 page9.00 M Internal Road 9.00 M Internal Road: Water BodyRichaNo ratings yet
- 9.00 M Internal Road 9.00 M Internal Road: Water Body - 1.2 M LVL Water Body - 1.2 M LVLDocument1 page9.00 M Internal Road 9.00 M Internal Road: Water Body - 1.2 M LVL Water Body - 1.2 M LVLRichaNo ratings yet
- Children Bedroom Nashik: Furniture Plan Electrical PlanDocument1 pageChildren Bedroom Nashik: Furniture Plan Electrical PlanRichaNo ratings yet
- Oral Malodor: Nidhi Sharma InternDocument21 pagesOral Malodor: Nidhi Sharma InternRichaNo ratings yet
- Class I Class Ii: Nidhi Sharma InternDocument1 pageClass I Class Ii: Nidhi Sharma InternRichaNo ratings yet
- 3ard - 01 SopDocument1 page3ard - 01 SopRichaNo ratings yet
- Centre Line Plan: Schedule of ColumnsDocument1 pageCentre Line Plan: Schedule of ColumnsRichaNo ratings yet
- Basement Floor Plan: Extraction Room 130 SQ.MDocument1 pageBasement Floor Plan: Extraction Room 130 SQ.MRichaNo ratings yet
- 03 Foundation PlanDocument1 page03 Foundation PlanRichaNo ratings yet
- Key Plan: Plan of Kitchen Plan of Kitchen at 2'-0" LVLDocument1 pageKey Plan: Plan of Kitchen Plan of Kitchen at 2'-0" LVLRichaNo ratings yet
- Detail of Common Toilet: Section Elevation C - C' Section Elevation D - D'Document1 pageDetail of Common Toilet: Section Elevation C - C' Section Elevation D - D'RichaNo ratings yet
- The Early Signs of Malocclusion: B. C. LeightonDocument7 pagesThe Early Signs of Malocclusion: B. C. LeightonEstaf EmkeyzNo ratings yet
- Skala Prilaku FranklDocument6 pagesSkala Prilaku FranklMeta Anjany FirmansyahNo ratings yet
- A Comparison of Human Dental Pulp Response To CalcDocument5 pagesA Comparison of Human Dental Pulp Response To CalcrespikNo ratings yet
- Smile Volume 3 Issue 4Document69 pagesSmile Volume 3 Issue 4Jack ChiouNo ratings yet
- Esthetic Dentistry / Orthodontic Courses by Indian Dental AcademyDocument256 pagesEsthetic Dentistry / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- The Combination Syndrome ' Revisited PDFDocument7 pagesThe Combination Syndrome ' Revisited PDFRamona MateiNo ratings yet
- Sterilization of Ortho Instruments / Orthodontic Courses by Indian Dental AcademyDocument57 pagesSterilization of Ortho Instruments / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Caries Theory PDFDocument21 pagesCaries Theory PDFAlex KwokNo ratings yet
- Thomas Levy PDFDocument18 pagesThomas Levy PDFsusan64100% (3)
- E2O Dental Waterline Treatment Sell Sheet 2013Document2 pagesE2O Dental Waterline Treatment Sell Sheet 2013JandT Dental TradingNo ratings yet
- Flat Ridgel Impression TechniqueDocument4 pagesFlat Ridgel Impression TechniquerekabiNo ratings yet
- Optimization of Emergence Profile of Implant ProstDocument8 pagesOptimization of Emergence Profile of Implant ProstAya Ibrahim YassinNo ratings yet
- BleachingDocument62 pagesBleachingوردة صبرNo ratings yet
- Root Canal Anatomy of Human TeethDocument11 pagesRoot Canal Anatomy of Human TeethGorgi KostovNo ratings yet
- 2 - Ricketts CephalometryDocument294 pages2 - Ricketts Cephalometrynhasuonline100% (2)
- H2022011 - Bhumika Gupta - CV - Soumya BanerjeeDocument1 pageH2022011 - Bhumika Gupta - CV - Soumya Banerjeeabhay SaxenaNo ratings yet
- Endodontic Treatment With 3mix-MpDocument7 pagesEndodontic Treatment With 3mix-MpSergio Llufire MendozaNo ratings yet
- Class V. Cavity PreparationDocument44 pagesClass V. Cavity PreparationShahid HameedNo ratings yet
- TeethDocument17 pagesTeethSheryce Gwyneth GuadalupeNo ratings yet
- Mucogingival Surgery IDocument32 pagesMucogingival Surgery IMayleen LeeNo ratings yet
- Immediate Dentin Sealing of Onlay Preparations - Thickness of Pre-Cured Dentin Bonding Agent and Effect of Surface CleaningDocument11 pagesImmediate Dentin Sealing of Onlay Preparations - Thickness of Pre-Cured Dentin Bonding Agent and Effect of Surface CleaningIlias100% (1)
- Failure of Amalgam Restoration PDFDocument2 pagesFailure of Amalgam Restoration PDFJaime0% (1)
- Rosen 1961Document14 pagesRosen 1961Fer TorresNo ratings yet
- Predicting The Wits Appraisal From The ANB AngleDocument7 pagesPredicting The Wits Appraisal From The ANB AngleMarlene TopeteNo ratings yet
- Removable Partial Dentures: The Clinical Need For InnovationDocument8 pagesRemovable Partial Dentures: The Clinical Need For InnovationNetra TaleleNo ratings yet
- Ca 2015 24Document36 pagesCa 2015 24singh1699No ratings yet
- Medical EducationDocument7 pagesMedical EducationnmukievNo ratings yet
- Oral Implantology: ImplantsDocument52 pagesOral Implantology: ImplantsDabala Harish Reddy100% (6)
- Quick A - E F S B: Irway Sthetics - Unction - Tructure - IologyDocument1 pageQuick A - E F S B: Irway Sthetics - Unction - Tructure - IologyChrisNo ratings yet
- Biologic WidthDocument44 pagesBiologic WidthRohit Rai100% (2)