You might also like
- Necrotizing Enterocolitis: Reproduction System 2010Document39 pagesNecrotizing Enterocolitis: Reproduction System 2010GilankNo ratings yet
- Necrotizing Enterocolitis: Reproduction System 2010Document39 pagesNecrotizing Enterocolitis: Reproduction System 2010Anonymous Af24L7No ratings yet
- Necrotizing EnterocolitisDocument43 pagesNecrotizing EnterocolitisRajender SinghNo ratings yet
- Necrotizing EnterocolitisDocument24 pagesNecrotizing Enterocolitisfadhila khairunnisaNo ratings yet
- VolvulusDocument38 pagesVolvulusHector RaulNo ratings yet
- Neonatal Acute Abdomen. 7th YrDocument54 pagesNeonatal Acute Abdomen. 7th YrFreeburn SimunchembuNo ratings yet
- Necrotizing Enterocolitis: Janice Nicklay Catalan M.DDocument27 pagesNecrotizing Enterocolitis: Janice Nicklay Catalan M.DrianurjanahNo ratings yet
- DR A S KumarDocument41 pagesDR A S KumardrmkumarNo ratings yet
- Colon, Rectum and AnusDocument30 pagesColon, Rectum and AnusKiara GovenderNo ratings yet
- Necrotizing Enterocolitis (NEC) : Intensive Care Nursery House Staff ManualDocument3 pagesNecrotizing Enterocolitis (NEC) : Intensive Care Nursery House Staff ManualJovvitaNo ratings yet
- Surgical AbdomenDocument3 pagesSurgical Abdomendude dNo ratings yet
- Necrotising Enterocolitis (NEC) : Clinical Practice Guideline Guideline Coverage Includes NICU KEMH, NICU PMH and NETS WADocument3 pagesNecrotising Enterocolitis (NEC) : Clinical Practice Guideline Guideline Coverage Includes NICU KEMH, NICU PMH and NETS WAemilly vidyaNo ratings yet
- Necrotizing Enterocolitis: Janice Nicklay Catalan M.DDocument27 pagesNecrotizing Enterocolitis: Janice Nicklay Catalan M.DLaurensia Erlina NataliaNo ratings yet
- Necrotizing Enterocolitis ProtocolDocument3 pagesNecrotizing Enterocolitis Protocoleddy riachyNo ratings yet
- Management of Clients With Intestinal Disorders: - Michael D. Manglapus, BSN-RN, RM, MANDocument101 pagesManagement of Clients With Intestinal Disorders: - Michael D. Manglapus, BSN-RN, RM, MANMichael Baylon DueñasNo ratings yet
- Pead 3 - Abdominal Pain and VommitingDocument22 pagesPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- Necrotizing EnterocolitisDocument36 pagesNecrotizing EnterocolitisMahad Maxamed AxmedNo ratings yet
- ACUTE ABDOMEN-Approach To Managment-HazemDocument57 pagesACUTE ABDOMEN-Approach To Managment-HazemMohamed Hazem ElfollNo ratings yet
- Nursing Stomach NotesDocument5 pagesNursing Stomach Noteslucas dibenedettoNo ratings yet
- Ipi 82603Document18 pagesIpi 82603Megawati LiwangNo ratings yet
- DDX of RIF Mass (Syazwani)Document44 pagesDDX of RIF Mass (Syazwani)Nurul Syazwani RamliNo ratings yet
- Imaging Acute Abdomen DR - Rivani Kurniawan FixDocument86 pagesImaging Acute Abdomen DR - Rivani Kurniawan FixRivani KurniawanNo ratings yet
- Biliary System and Pancreatic DisorderDocument59 pagesBiliary System and Pancreatic DisorderAlda AdeliaNo ratings yet
- PeritonitisDocument20 pagesPeritonitisYasirNo ratings yet
- Acute Abdomen: Part I: Intestinal Obstruction/Bowel Infarction/ Constipation (And How To Assess and Initiate Management)Document63 pagesAcute Abdomen: Part I: Intestinal Obstruction/Bowel Infarction/ Constipation (And How To Assess and Initiate Management)Rumana IslamNo ratings yet
- Appendicitis 5.9Document50 pagesAppendicitis 5.9Smart SaravanaNo ratings yet
- 1100 Ultrasound of The Acute Abdomen 15 3Document84 pages1100 Ultrasound of The Acute Abdomen 15 3gp1promo2016No ratings yet
- Approach To Abdominal Pain in EDDocument29 pagesApproach To Abdominal Pain in EDAneeq Nayer KhanNo ratings yet
- Necrotizing EnterocolitisDocument31 pagesNecrotizing EnterocolitisRas Siko SafoNo ratings yet
- PERITONITISDocument12 pagesPERITONITISHayat AL AKOUM100% (1)
- Nec 2018Document33 pagesNec 2018Abraham AnaelyNo ratings yet
- Appendix ModuleDocument30 pagesAppendix ModuleNagulan ChanemougameNo ratings yet
- PANCREASDocument74 pagesPANCREASzaiba0786No ratings yet
- Pemicu 5Document75 pagesPemicu 5Cantika Monica LonanNo ratings yet
- Abdominal Distention inDocument45 pagesAbdominal Distention inArif Rahman DmNo ratings yet
- Acute PancreatitisDocument79 pagesAcute Pancreatitiszaiba0786No ratings yet
- Dr. H. Achmad Fuadi, SPB-KBD, MkesDocument47 pagesDr. H. Achmad Fuadi, SPB-KBD, MkesytreiiaaNo ratings yet
- Congenital Hypertrophic Pyloric Stenosis: Dr. Kundan Department of Surgery Patna Medical College & HospitalDocument17 pagesCongenital Hypertrophic Pyloric Stenosis: Dr. Kundan Department of Surgery Patna Medical College & HospitalChamika HuruggamuwaNo ratings yet
- Bile, Bile Duct and Pancreatic DiseaseDocument82 pagesBile, Bile Duct and Pancreatic Diseaseshahrul rahmanNo ratings yet
- Intestinal Obstruction...Document26 pagesIntestinal Obstruction...Yonathan asnakeNo ratings yet
- Pedia Surg Module, Grp11&2Document91 pagesPedia Surg Module, Grp11&2Jelyn ManipisNo ratings yet
- Acute Appendicitis by DR.S.HDocument24 pagesAcute Appendicitis by DR.S.Hkevinharahap26No ratings yet
- Acute Abdomen: - DefinitionDocument27 pagesAcute Abdomen: - DefinitionWorku KifleNo ratings yet
- GIS-K-25 Acute Appendicitis Appendiceal Mass / AbscessDocument24 pagesGIS-K-25 Acute Appendicitis Appendiceal Mass / AbscessYasmine Fitrina SiregarNo ratings yet
- IntussusceptionDocument14 pagesIntussusceptionAmit RamrattanNo ratings yet
- NECDocument32 pagesNECettevyviNo ratings yet
- Bowel ObstructionDocument48 pagesBowel ObstructionPatrick John100% (1)
- Problem 4 GITDocument94 pagesProblem 4 GITArioNo ratings yet
- Acute AbdomenDocument36 pagesAcute AbdomenAdriani NadhirahNo ratings yet
- Pancreatitis Ercp Pain Amylase Lipase ErcpDocument24 pagesPancreatitis Ercp Pain Amylase Lipase ErcpPerplexed CeleryNo ratings yet
- K-25 Acute AppendicitisDocument23 pagesK-25 Acute AppendicitiscarinasheliapNo ratings yet
- AppendicitisDocument27 pagesAppendicitiskarenelijah147No ratings yet
- Cme Acute AbdomenDocument110 pagesCme Acute AbdomenGregory JamesNo ratings yet
- Small Bowel ObstructionDocument38 pagesSmall Bowel ObstructionRUSSELL CILOTNo ratings yet
- Intestinal ObstructionDocument52 pagesIntestinal ObstructionAsfandyar Khan100% (2)
- Diverticular Disease 2Document5 pagesDiverticular Disease 2karl abiaadNo ratings yet
- Acute Abdominal Pain: Dr. Putra Hendra SPPD UnibaDocument43 pagesAcute Abdominal Pain: Dr. Putra Hendra SPPD UnibaDian PuspaNo ratings yet
- Learning Objective: - Explain of Acute AbdomenDocument143 pagesLearning Objective: - Explain of Acute AbdomenSamuel Sebastian SirapanjiNo ratings yet
- Acute Abdominal Pain: DR Naing Naing Oo Senior LecturerDocument28 pagesAcute Abdominal Pain: DR Naing Naing Oo Senior LecturerAbdulrahman NajiNo ratings yet
- Prevenção Secundária Avc Isquêmico - Guideline 2022Document41 pagesPrevenção Secundária Avc Isquêmico - Guideline 2022Felipe Stoquetti de AbreuNo ratings yet
- Post Traumatic Stress DisorderDocument4 pagesPost Traumatic Stress DisorderaploureyNo ratings yet
- 7985 - Jadwal GIS 1920Document12 pages7985 - Jadwal GIS 1920amelia rahayuNo ratings yet
- NGT Ogt-FeedingDocument14 pagesNGT Ogt-Feedingnibbles nibblesNo ratings yet
- Journal Reading RPL EditDocument30 pagesJournal Reading RPL EditAnonymous l6Q1ROq2No ratings yet
- G02-Assessment, Management and Decision Making in The Treatment of Polytrauma Patients With Head InjuriesDocument55 pagesG02-Assessment, Management and Decision Making in The Treatment of Polytrauma Patients With Head Injurieskosmynin86No ratings yet
- Kidney DiseasesDocument93 pagesKidney DiseasesDoreen NNo ratings yet
- ParalysisDocument4 pagesParalysissakuraleeshaoranNo ratings yet
- Anaemia in Pregnancy: Klinik Kesihatan Ibu Dan Anak Parit BuntarDocument10 pagesAnaemia in Pregnancy: Klinik Kesihatan Ibu Dan Anak Parit Buntarannurshah05No ratings yet
- Important Instructions For Pre-Employment Medical TestDocument2 pagesImportant Instructions For Pre-Employment Medical TestAnjali KumariNo ratings yet
- Valproic Acid DsDocument2 pagesValproic Acid DsCarissa Mae Tapec EstradaNo ratings yet
- Vigabatrin For IsDocument12 pagesVigabatrin For IsAndrew SantosoNo ratings yet
- Behavior and Mental Status Can Be Early Signs of Impaired Gas ExchangeDocument2 pagesBehavior and Mental Status Can Be Early Signs of Impaired Gas ExchangeJoanna Marie Lumbre BalbiranNo ratings yet
- 0199975744Document305 pages0199975744nicoletaelenaNo ratings yet
- MCQ-Chronic Obstructive Pulmonary DiseaseDocument3 pagesMCQ-Chronic Obstructive Pulmonary DiseaseMittulNo ratings yet
- TB in Special SituationsDocument49 pagesTB in Special SituationsVipul KumarNo ratings yet
- Hernia - Surgery PrecisDocument1 pageHernia - Surgery PrecisSherif WagdyNo ratings yet
- Anatomic Therapy PDFDocument364 pagesAnatomic Therapy PDFrahul_choubey_9No ratings yet
- Therapy of Acute Respiratory Infections in Children: NoveltiesDocument11 pagesTherapy of Acute Respiratory Infections in Children: NoveltiesrizkaNo ratings yet
- PONR - Comprehensive Nursing Health History and Physical ExaminationDocument21 pagesPONR - Comprehensive Nursing Health History and Physical ExaminationDRJC100% (1)
- Check Unit 555 November Immunology V3 PDFDocument25 pagesCheck Unit 555 November Immunology V3 PDFdragon66No ratings yet
- Examination EntDocument7 pagesExamination EntNadz RlanNo ratings yet
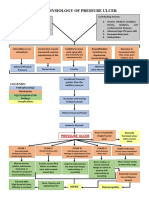
- Pathophysiology of Pressure UlcerDocument1 pagePathophysiology of Pressure UlcerSTORAGE FILENo ratings yet
- POULTRY PATHO - Marek's DiseaseDocument31 pagesPOULTRY PATHO - Marek's DiseaseArooma KhalidNo ratings yet
- Case Study On Nephrotic SyndromeDocument7 pagesCase Study On Nephrotic SyndromeArchana VermaNo ratings yet
- A Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Document13 pagesA Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Samantha BolanteNo ratings yet
- Cerebral Salt Wasting SyndromeDocument6 pagesCerebral Salt Wasting SyndromeAbi ArifiNo ratings yet
- Metformin, Glucophage, Glucophage XR, Glumetza, Fortamet, RiometDocument5 pagesMetformin, Glucophage, Glucophage XR, Glumetza, Fortamet, RiometAgronaSlaughterNo ratings yet
- Alternative Health & Herbs Remedies 425 Jackson SE, Albany, OR 97321 1-541-791-8400Document159 pagesAlternative Health & Herbs Remedies 425 Jackson SE, Albany, OR 97321 1-541-791-8400Marvin T Verna100% (2)
- JH CERILLES STATE COLLEGE - Post TestDocument7 pagesJH CERILLES STATE COLLEGE - Post TestCrystal Ann TadiamonNo ratings yet