You might also like
- Cyclosporine Clinical Uses, Dosage, Monitoring & InteractionsDocument24 pagesCyclosporine Clinical Uses, Dosage, Monitoring & Interactionssanchit_J14No ratings yet
- TDM: Cyclosporin: Course: Advanced Clinical Pharmacy Corse No 711-T Course Incharge: Saima Saleem (Assistant Professor)Document11 pagesTDM: Cyclosporin: Course: Advanced Clinical Pharmacy Corse No 711-T Course Incharge: Saima Saleem (Assistant Professor)Samra KhanNo ratings yet
- FluconazoleDocument3 pagesFluconazoleapi-3797941100% (1)
- Cefuroxime: Cephalosporins See Available Brands of Cefuroxime See Related Cefuroxime InformationDocument3 pagesCefuroxime: Cephalosporins See Available Brands of Cefuroxime See Related Cefuroxime InformationKarmelaCosonNo ratings yet
- PP ObatDocument7 pagesPP ObatSaifan AbdurrohmanNo ratings yet
- Cyclosporin Final (1) - 1-EditDocument32 pagesCyclosporin Final (1) - 1-Editsky.blueNo ratings yet
- Cefazolin AncefDocument4 pagesCefazolin AncefAmanda La SalaNo ratings yet
- 07 Miscellaneous Drugs Group ADocument64 pages07 Miscellaneous Drugs Group AKamal GhimireNo ratings yet
- CiproflaxacinDocument3 pagesCiproflaxacindonnas1128No ratings yet
- 019537s074,020780s032lbl PDFDocument42 pages019537s074,020780s032lbl PDFLinawati Nurannisa PutriNo ratings yet
- Prescribing Information: 1. Name of The Medicinal ProductDocument5 pagesPrescribing Information: 1. Name of The Medicinal Productddandan_20% (1)
- Ciproflaxin Drug CardDocument2 pagesCiproflaxin Drug CardRaenell CurryNo ratings yet
- CiclosporinDocument7 pagesCiclosporinLunatic DreamerNo ratings yet
- LevofloxacinDocument3 pagesLevofloxacinapi-3797941100% (2)
- Data Sheet: VesicareDocument10 pagesData Sheet: VesicareumarNo ratings yet
- Clostridium Difficile Guideline - UMMCDocument5 pagesClostridium Difficile Guideline - UMMCdamondouglas100% (3)
- Lincomycin HydrochlorideDocument1 pageLincomycin HydrochlorideDiego TorresNo ratings yet
- Pyra TBDocument6 pagesPyra TBRaya Ibarra LumogdangNo ratings yet
- 3.E.2-Caspofungin Guideline 2003Document3 pages3.E.2-Caspofungin Guideline 2003damondouglasNo ratings yet
- Chronic Renal Failure During PregnancyDocument42 pagesChronic Renal Failure During PregnancyvincentsharonNo ratings yet
- ImunosupresanDocument37 pagesImunosupresanadezaNo ratings yet
- Myrin P ForteDocument3 pagesMyrin P ForteJohn Zedric Villanueva ArciagaNo ratings yet
- Keto LogDocument7 pagesKeto LogKim Justin InfantadoNo ratings yet
- Ciprobay PIDocument21 pagesCiprobay PIJing Yi LeongNo ratings yet
- 019537s082 020780s040lbl PDFDocument43 pages019537s082 020780s040lbl PDFShahab Ud DinNo ratings yet
- CRF in PregnancyDocument27 pagesCRF in PregnancyJitendra AgrawalNo ratings yet
- Therapeutic and Toxic ConcentrationsDocument8 pagesTherapeutic and Toxic ConcentrationsReyadh JassemNo ratings yet
- Drug StudyDocument8 pagesDrug StudyLea FestejoNo ratings yet
- Tishk International University: ApixabanDocument4 pagesTishk International University: ApixabanDyar MzafarNo ratings yet
- Drug Monograph: Generic Name: Trade Name: Drug Class: IndicationsDocument10 pagesDrug Monograph: Generic Name: Trade Name: Drug Class: IndicationsRawan AlmutairiNo ratings yet
- AntibioticsDocument58 pagesAntibioticsKamal GhimireNo ratings yet
- Approach ConsiderationsDocument12 pagesApproach ConsiderationsTyna Mew-mewNo ratings yet
- Pharmacotherapeutics-1 Assignment: SelinexorDocument20 pagesPharmacotherapeutics-1 Assignment: SelinexorRobert Selvin MNo ratings yet
- Drug StudyDocument8 pagesDrug Studymaryhiromi10No ratings yet
- Cloxacillin and inDocument6 pagesCloxacillin and inGabb CabigtingNo ratings yet
- Levofloxacin 500mg Film-coated Tablets SmPC SummaryDocument10 pagesLevofloxacin 500mg Film-coated Tablets SmPC SummaryOdunlamiNo ratings yet
- Metoclopramide Generic Medicine InfoDocument7 pagesMetoclopramide Generic Medicine InfoRasco, Allen jayNo ratings yet
- Targocid Product InformationDocument5 pagesTargocid Product InformationAsto Ata InteristiNo ratings yet
- Metoclopramide: GIT Regulators, Antiflatulents & Anti-Inflammatories Antiemetics See Available Brands of MetoclopramideDocument9 pagesMetoclopramide: GIT Regulators, Antiflatulents & Anti-Inflammatories Antiemetics See Available Brands of MetoclopramideDominique RamosNo ratings yet
- Metoclopramide uses and dosageDocument9 pagesMetoclopramide uses and dosageDominique RamosNo ratings yet
- Drug Study for Hepatic Abscess PatientDocument3 pagesDrug Study for Hepatic Abscess PatientEric EvangelistaNo ratings yet
- Hormonal Contraception: Oral, Parenteral and Implanted ContraceptivesDocument14 pagesHormonal Contraception: Oral, Parenteral and Implanted ContraceptivesFrancia ToledanoNo ratings yet
- CyclophosphamideDocument2 pagesCyclophosphamideksumanpharma8801No ratings yet
- Nephrotic Syndrome Treatment & Management - Approach Considerations, Acute NephroDocument5 pagesNephrotic Syndrome Treatment & Management - Approach Considerations, Acute NephroErvirson Jair Cañon AbrilNo ratings yet
- Classification (S) Therapeutic: Anti-Infectives Pharmacologic: FluoroquinolonesDocument9 pagesClassification (S) Therapeutic: Anti-Infectives Pharmacologic: FluoroquinolonesFildehl Janice Bomediano CatipayNo ratings yet
- Cipro: (Ciprofloxacin Hydrochloride) TabletsDocument31 pagesCipro: (Ciprofloxacin Hydrochloride) Tabletskichi_atsukaiNo ratings yet
- Cyclosporine PDFDocument6 pagesCyclosporine PDFFazdrah AssyuaraNo ratings yet
- Availability: Ciprofloxacin Hydrochloride Ciprofloxacin OphthalmicDocument4 pagesAvailability: Ciprofloxacin Hydrochloride Ciprofloxacin OphthalmicCay SevillaNo ratings yet
- Hyper Emesis GravidarumDocument22 pagesHyper Emesis Gravidarumchandu ranaNo ratings yet
- Bruce Raymond L. Juele BSN 2-DDocument36 pagesBruce Raymond L. Juele BSN 2-DAno NymousNo ratings yet
- Drug Monograph: Generic Name: Trade Name: Drug Class: IndicationsDocument8 pagesDrug Monograph: Generic Name: Trade Name: Drug Class: IndicationsRawan AlmutairiNo ratings yet
- Ibs FinalDocument71 pagesIbs FinalSaktai DiyamiNo ratings yet
- Antibiotik Dan Antiseptik Saluran KemihDocument29 pagesAntibiotik Dan Antiseptik Saluran KemihPutri Sari SeptirianiNo ratings yet
- Gout and HyperuricemiaDocument7 pagesGout and HyperuricemiaTaj lamajedNo ratings yet
- Description:: Assignment On MifepristoneDocument5 pagesDescription:: Assignment On Mifepristonevenkata samyukthaNo ratings yet
- Con 1420782810247Document7 pagesCon 1420782810247AsetonitrileNo ratings yet
- Annex I Summary of Product CharacteristicsDocument60 pagesAnnex I Summary of Product CharacteristicsMadhu MitaNo ratings yet
- Neomycin Is An Aminoglycoside AntibioticDocument5 pagesNeomycin Is An Aminoglycoside AntibioticDeby Nareswari HuslanNo ratings yet
- 1.CBE CME Obstructive JaundiceDocument39 pages1.CBE CME Obstructive JaundicedeepikaNo ratings yet
- Buffers and PH Adjusting AgentsDocument8 pagesBuffers and PH Adjusting AgentsJoão SantosNo ratings yet
- Alda Risma CaseDocument13 pagesAlda Risma CasealdiraNo ratings yet
- Anne Marbun CaseDocument16 pagesAnne Marbun CasealdiraNo ratings yet
- Alda Risma CaseDocument13 pagesAlda Risma CasealdiraNo ratings yet
- AFP Mechanism of Nephrotoxic DrugsDocument9 pagesAFP Mechanism of Nephrotoxic DrugsaldiraNo ratings yet
- Opioid AnalgesicDocument10 pagesOpioid AnalgesicaldiraNo ratings yet
- SimmonsDocument12 pagesSimmonsGürelBaltalıNo ratings yet
- Information Security Management System: Gheorghe MirelaDocument6 pagesInformation Security Management System: Gheorghe MirelaChristen CastilloNo ratings yet
- Let's Check: To Eliminate Unrealized Gain On Sale of LandDocument4 pagesLet's Check: To Eliminate Unrealized Gain On Sale of Landalmira garciaNo ratings yet
- Pearly Co Cleared Funds ForecastDocument8 pagesPearly Co Cleared Funds ForecastPutin Phy0% (1)
- Cat Helimax 2016 Esp 1Document74 pagesCat Helimax 2016 Esp 1HKM IngenierosNo ratings yet
- Ni 2 WordDocument2 pagesNi 2 WordLeigh Angelika Dela CruzNo ratings yet
- SordariaDocument31 pagesSordariaapi-251288828No ratings yet
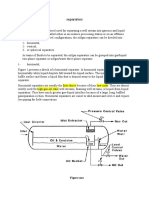
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)
- M&SDocument39 pagesM&Sgo.pushp70910% (1)
- RESOLUTION 2022-08 Denial of Setback VarianceDocument5 pagesRESOLUTION 2022-08 Denial of Setback VarianceMatt McKinneyNo ratings yet
- Hyundai forklift specification dimensionsDocument6 pagesHyundai forklift specification dimensionsАлександр ОлейникNo ratings yet
- Bibliometric Handbook For Karolinska InstitutetDocument41 pagesBibliometric Handbook For Karolinska InstitutetCamila Araya G100% (1)
- Miller Toyota-Conversion-Kit Letter ENG WEBDocument4 pagesMiller Toyota-Conversion-Kit Letter ENG WEBskyduckNo ratings yet
- InfraTapp - Infra Tapp - Manual ENGDocument64 pagesInfraTapp - Infra Tapp - Manual ENGEliaNo ratings yet
- MMDST PDFDocument50 pagesMMDST PDFChristopher OlipasNo ratings yet
- Land Tenure SystemsDocument140 pagesLand Tenure SystemsjoeclintNo ratings yet
- Waleed Alomari CVDocument2 pagesWaleed Alomari CValomari_waleedNo ratings yet
- California ProfileDocument3 pagesCalifornia ProfileLigaya BacuelNo ratings yet
- IED Recognition GuideDocument28 pagesIED Recognition GuideLeafs61100% (5)
- Accessibility POC: October 26, 2017Document7 pagesAccessibility POC: October 26, 2017Ramesh BodukaniNo ratings yet
- Old Fashioned Southern Tea CakesDocument2 pagesOld Fashioned Southern Tea CakesDB ScottNo ratings yet
- FarkolDocument7 pagesFarkolHasiadin LaodeNo ratings yet
- Laughter Yoga Benefits Workplace ProductivityDocument2 pagesLaughter Yoga Benefits Workplace ProductivityJose Manuel Araujo OrregoNo ratings yet
- FD2000 DatasheetDocument2 pagesFD2000 DatasheetIvan MihajlovicNo ratings yet
- Literature Review On Procrastination Impact On Academic PerformanceDocument2 pagesLiterature Review On Procrastination Impact On Academic Performancemomi100% (1)
- PCS-9656 Arc ProtectionDocument3 pagesPCS-9656 Arc ProtectionganeshNo ratings yet
- Fujitsu GeneralDocument51 pagesFujitsu GeneralZubair DarNo ratings yet
- Folder Hexa EngDocument8 pagesFolder Hexa EngMuresan MVNo ratings yet
- Solving Proportions Problems with Learning Activity SheetsDocument21 pagesSolving Proportions Problems with Learning Activity Sheetsceline fernandezNo ratings yet
- Paper 1Document8 pagesPaper 1Santhoshi Sadhanaa SankarNo ratings yet