You might also like
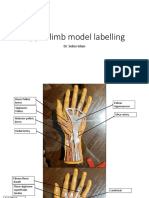
- Upper Limb Model Labelling PDFDocument11 pagesUpper Limb Model Labelling PDFSana AftabNo ratings yet
- Infections of Female Genital TractDocument67 pagesInfections of Female Genital TractSana AftabNo ratings yet
- Surface Anatomy PDFDocument90 pagesSurface Anatomy PDFSana AftabNo ratings yet
- Power of Lower Limb: DR - Tayyeba Iftikhar Mirza Senior Lecturer DMEDocument12 pagesPower of Lower Limb: DR - Tayyeba Iftikhar Mirza Senior Lecturer DMESana AftabNo ratings yet
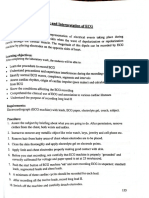
- Ecg 4TH JuneDocument227 pagesEcg 4TH JuneSana AftabNo ratings yet
- Grand 50 Mixed MCQS (Part-1)Document16 pagesGrand 50 Mixed MCQS (Part-1)Sana AftabNo ratings yet
- Grand 50 Mixed MCQS (Part-3)Document17 pagesGrand 50 Mixed MCQS (Part-3)Sana AftabNo ratings yet
- Upper Limb Model LabellingDocument11 pagesUpper Limb Model LabellingSana AftabNo ratings yet
- Net Iq Portion (Part-8)Document35 pagesNet Iq Portion (Part-8)Sana AftabNo ratings yet
- Physio PracticalsDocument22 pagesPhysio PracticalsSana AftabNo ratings yet
- Surface AnatomyDocument90 pagesSurface AnatomySana AftabNo ratings yet
- New Doc 04-11-2020 18.32.09Document5 pagesNew Doc 04-11-2020 18.32.09Sana AftabNo ratings yet
- PHYSICSDocument2 pagesPHYSICSSana AftabNo ratings yet
- Chapter 15 Electronic-Om AmpDocument51 pagesChapter 15 Electronic-Om AmpSana AftabNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Faculty of Computer Science and Information TechnologyDocument4 pagesFaculty of Computer Science and Information TechnologyNurafiqah Sherly Binti ZainiNo ratings yet
- Developmental PsychologyDocument2 pagesDevelopmental PsychologyPatricia Xandra AurelioNo ratings yet
- Wa0009.Document14 pagesWa0009.Pradeep SinghNo ratings yet
- Schopenhauer and KantDocument8 pagesSchopenhauer and KantshawnNo ratings yet
- Effect of Perceived Work Environment On Employees' Job Behaviour and Organizational EffectivenessDocument10 pagesEffect of Perceived Work Environment On Employees' Job Behaviour and Organizational EffectivenessTanvee SharmaNo ratings yet
- Romeuf Et Al., 1995Document18 pagesRomeuf Et Al., 1995David Montaño CoronelNo ratings yet
- Planning and Design of A Cricket StadiumDocument14 pagesPlanning and Design of A Cricket StadiumTenu Sara Thomas50% (6)
- MoMA Learning Design OverviewDocument28 pagesMoMA Learning Design OverviewPenka VasilevaNo ratings yet
- Nota 4to Parcial ADocument8 pagesNota 4to Parcial AJenni Andrino VeNo ratings yet
- Atividade de InglêsDocument8 pagesAtividade de InglêsGabriel FreitasNo ratings yet
- Fort St. John 108 Street & Alaska Highway IntersectionDocument86 pagesFort St. John 108 Street & Alaska Highway IntersectionAlaskaHighwayNewsNo ratings yet
- Pedia Edited23 PDFDocument12 pagesPedia Edited23 PDFAnnJelicaAbonNo ratings yet
- 413 14 Speakout Upper Intermediate 2nd Tests With Key and ScriptDocument158 pages413 14 Speakout Upper Intermediate 2nd Tests With Key and ScriptHal100% (2)
- Café Management System Full and Final ReportDocument18 pagesCafé Management System Full and Final ReportMuhammad Xalman Xhaw100% (3)
- Apply Study and Learning SkillsDocument58 pagesApply Study and Learning SkillsSelf-DeveloperNo ratings yet
- Rapidjson Library ManualDocument79 pagesRapidjson Library ManualSai Kumar KvNo ratings yet
- COSMO NEWS September 1, 2019 EditionDocument4 pagesCOSMO NEWS September 1, 2019 EditionUnited Church of Christ in the PhilippinesNo ratings yet
- Independence of Costa RicaDocument2 pagesIndependence of Costa Ricaangelica ruizNo ratings yet
- NURS 366 Exam 1 Study Guide and RubricDocument7 pagesNURS 366 Exam 1 Study Guide and RubriccmpNo ratings yet
- Checklist of Requirements of Special Land Use PermitDocument1 pageChecklist of Requirements of Special Land Use PermitAnghelita ManaloNo ratings yet
- Accaf3junwk3qa PDFDocument13 pagesAccaf3junwk3qa PDFTiny StarsNo ratings yet
- Court Documents From Toronto Police Project Brazen - Investigation of Alexander "Sandro" Lisi and Toronto Mayor Rob FordDocument474 pagesCourt Documents From Toronto Police Project Brazen - Investigation of Alexander "Sandro" Lisi and Toronto Mayor Rob Fordanna_mehler_papernyNo ratings yet
- OatDocument46 pagesOatHari BabuNo ratings yet
- Chronology of Events:: Account: North Davao Mining Corp (NDMC)Document2 pagesChronology of Events:: Account: North Davao Mining Corp (NDMC)John Robert BautistaNo ratings yet
- Myocardial Concept MappingDocument34 pagesMyocardial Concept MappingTHIRD YEARNo ratings yet
- Gender CriticismDocument17 pagesGender CriticismJerickRepilRabeNo ratings yet
- Indian School Bousher Final Term End Exam (T2) : Academic Session - 2021-22 Grade: 7Document7 pagesIndian School Bousher Final Term End Exam (T2) : Academic Session - 2021-22 Grade: 7Shresthik VenkateshNo ratings yet
- CBDCs For Dummies Everything You Need ToDocument18 pagesCBDCs For Dummies Everything You Need Tolati.training7No ratings yet
- PMP Chapter-12 P. Procurement ManagementDocument30 pagesPMP Chapter-12 P. Procurement Managementashkar299No ratings yet
- FCI - GST - Manual On Returns and PaymentsDocument30 pagesFCI - GST - Manual On Returns and PaymentsAmber ChaturvediNo ratings yet