You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Bony OrbitDocument3 pagesThe Bony OrbitxxyumeNo ratings yet
- Shoulder Joint Anatomy GunaDocument65 pagesShoulder Joint Anatomy Gunakaradi2000No ratings yet
- Cervical Spine - Minimally Invasive and Open SurgeryDocument338 pagesCervical Spine - Minimally Invasive and Open Surgerymohamed lamrana jallohNo ratings yet
- FracturesDocument26 pagesFracturesMelinda MelinNo ratings yet
- TMJ SeminarDocument100 pagesTMJ SeminarMithileshwari Patil100% (1)
- Disorders of BonesDocument3 pagesDisorders of BonesAnonymous 0pSLjJYNo ratings yet
- The Diagram Below Represents An Unlabeled Skeleton. Which Part Does Each Number Represents?Document6 pagesThe Diagram Below Represents An Unlabeled Skeleton. Which Part Does Each Number Represents?smbdy tbhhhNo ratings yet
- Kinematics of Knee JointDocument16 pagesKinematics of Knee JointnttangNo ratings yet
- What Is The Skeletal System?Document21 pagesWhat Is The Skeletal System?Ezekiel A. NavarroNo ratings yet
- SkeletonDocument3 pagesSkeletonAngieNo ratings yet
- 3 - pg.51-113Document63 pages3 - pg.51-113api-3855624100% (1)
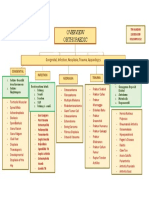
- Orthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesDocument1 pageOrthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesdinsNo ratings yet
- The Hip Joint (PDFDrive)Document492 pagesThe Hip Joint (PDFDrive)simona mariana dutuNo ratings yet
- Bone Grafting and Bone Graft SubstitutesDocument41 pagesBone Grafting and Bone Graft SubstitutesKiyasweet HaniNo ratings yet
- List of Skeletal Muscles of The Human Body - WikipediaDocument29 pagesList of Skeletal Muscles of The Human Body - WikipediaYoavNo ratings yet
- Posteroanterior Cephalometry: Craniofacial Frontal Analysis: Joseph G. GhafariDocument26 pagesPosteroanterior Cephalometry: Craniofacial Frontal Analysis: Joseph G. Ghafarisnes182No ratings yet
- Session 1 Hip and PelvisDocument62 pagesSession 1 Hip and PelvisNixon BiasNo ratings yet
- Surgical Orthopedics Anatomy Level 12 Spine Vertebral ColumnDocument48 pagesSurgical Orthopedics Anatomy Level 12 Spine Vertebral ColumnMustafa Kandil SolimanNo ratings yet
- Chapter 7 - CartilageDocument17 pagesChapter 7 - CartilageREMAN ALINGASANo ratings yet
- Anatomy of Head Subs Robert Acland AnatomyDocument8 pagesAnatomy of Head Subs Robert Acland AnatomysmohandesNo ratings yet
- 11 Biology Notes ch20 Locomotion and Movement PDFDocument3 pages11 Biology Notes ch20 Locomotion and Movement PDFRamachandranPerumalNo ratings yet
- Postnatal Growth and Development: Yenny Yustisia Dept. of Oral Biology Dentistry UNEJDocument38 pagesPostnatal Growth and Development: Yenny Yustisia Dept. of Oral Biology Dentistry UNEJMelisa Novitasari100% (1)
- Laboratory Manual For Anatomy and Physiology 6Th Edition Marieb Solutions Manual Full Chapter PDFDocument28 pagesLaboratory Manual For Anatomy and Physiology 6Th Edition Marieb Solutions Manual Full Chapter PDFJohnathanFitzgeraldnwoa100% (10)
- Injury Biomechanics: AAMIR SOHAIL - Student ID 163101039 - December 16, 2016Document12 pagesInjury Biomechanics: AAMIR SOHAIL - Student ID 163101039 - December 16, 2016Aamir SohailNo ratings yet
- Archery in The Meroitic Period New BioarDocument16 pagesArchery in The Meroitic Period New BioarGligor BozinoskiNo ratings yet
- LP. Nr.3 - Dr. IspasDocument4 pagesLP. Nr.3 - Dr. Ispasinna3003No ratings yet
- Support, Movement and LocomotionDocument3 pagesSupport, Movement and LocomotionAhmad Barrun Nidhom83% (23)
- Adult Equine (500Kg) - Increase KV or Mas If Cob/Warmblood or Very Swollen Decrease For Ponies or Young HorsesDocument1 pageAdult Equine (500Kg) - Increase KV or Mas If Cob/Warmblood or Very Swollen Decrease For Ponies or Young HorsesVengatNo ratings yet
- MODUL Praktikum Anatomi Dan HistologiDocument20 pagesMODUL Praktikum Anatomi Dan HistologiandikaNo ratings yet
- Joints of Axial SkeletonDocument24 pagesJoints of Axial SkeletonPraney SlathiaNo ratings yet