You might also like
- NAPLEX Practice Question Workbook: 1,000+ Comprehensive Practice Questions (2023 Edition)From EverandNAPLEX Practice Question Workbook: 1,000+ Comprehensive Practice Questions (2023 Edition)Rating: 4.5 out of 5 stars4.5/5 (3)
- Significant Early In-Hospital Benefit Was Seen. Clopidogrel Is Prefferd ToDocument8 pagesSignificant Early In-Hospital Benefit Was Seen. Clopidogrel Is Prefferd TogilnifNo ratings yet
- Cardiology: 27 Maret 2021Document52 pagesCardiology: 27 Maret 2021Dian ParamitaNo ratings yet
- Cardiology ReviewDocument10 pagesCardiology ReviewCooper Nikko ChavezNo ratings yet
- Cabg NursingDocument7 pagesCabg NursingDennis Cobb100% (1)
- Medical Management MI Heart AttackDocument9 pagesMedical Management MI Heart AttackTifanie Cyrine MerneloNo ratings yet
- ACC/AHA and ESC Guidelines for NSTEMI ManagementDocument10 pagesACC/AHA and ESC Guidelines for NSTEMI ManagementIboy ZulhamNo ratings yet
- Myocardial InfarctionDocument5 pagesMyocardial InfarctionNikki MacasaetNo ratings yet
- Acute Coronary Syndrome (ACS) Pathophysiology and TreatmentDocument39 pagesAcute Coronary Syndrome (ACS) Pathophysiology and TreatmentYowan SusantiNo ratings yet
- Case Scenarios Guide Differential Diagnosis and Management of Unstable AnginaDocument46 pagesCase Scenarios Guide Differential Diagnosis and Management of Unstable AnginaDemuel Dee L. BertoNo ratings yet
- Beta Blocker AgentsDocument28 pagesBeta Blocker Agentskuncupcupu1368No ratings yet
- Cardio Quiz Answer KeyDocument6 pagesCardio Quiz Answer KeyMark MasbadNo ratings yet
- Primary Care Management Following An Acute Myocardial InfarctionDocument4 pagesPrimary Care Management Following An Acute Myocardial InfarctionMaryjoy Gabriellee De La CruzNo ratings yet
- Management of Arrhythmias in The Cardiovascular Intensive Care UnitDocument15 pagesManagement of Arrhythmias in The Cardiovascular Intensive Care UnitGabriela PachecoNo ratings yet
- #3 Acs 6 PDFDocument6 pages#3 Acs 6 PDFOmar BasimNo ratings yet
- 2014 AHA SummaryDocument14 pages2014 AHA SummaryiamseraNo ratings yet
- Management of Unstable Angina/Non ST Elevation Myocardial Infarction (Ua/Nstemi) 2011Document40 pagesManagement of Unstable Angina/Non ST Elevation Myocardial Infarction (Ua/Nstemi) 2011Kokoland KukusNo ratings yet
- Cad CommerDocument2 pagesCad CommerWhatDoYouSeriesNo ratings yet
- Cardio BBDocument73 pagesCardio BBايات عبدالرحمنNo ratings yet
- FA InglesDocument4 pagesFA InglesDitzon EspinozaNo ratings yet
- Acs Coda KimbelDocument54 pagesAcs Coda KimbelJemsNo ratings yet
- Pulmonary Vascular Disease (TBL) : AcuteDocument3 pagesPulmonary Vascular Disease (TBL) : AcutetangledprincessNo ratings yet
- Step-2-Ck-Notes-Syrian-Student - HTML: Cardiology UWDocument15 pagesStep-2-Ck-Notes-Syrian-Student - HTML: Cardiology UWLoyla RoseNo ratings yet
- Esc Hypertrophic CardiomyopathyDocument9 pagesEsc Hypertrophic CardiomyopathyDheerajNo ratings yet
- Acetylsalicyclic Acid 08july2022Document6 pagesAcetylsalicyclic Acid 08july2022Cuong LeNo ratings yet
- Materi KardioDocument69 pagesMateri KardioDila AswitaliaNo ratings yet
- Acs 11 190524110746Document46 pagesAcs 11 190524110746Obakeng MandaNo ratings yet
- Review of Medical Treatment of Stable Ischemic Heart DiseaseDocument11 pagesReview of Medical Treatment of Stable Ischemic Heart DiseaseSuci NourmalizaNo ratings yet
- مذكرة أم القرى - النسخة 3Document431 pagesمذكرة أم القرى - النسخة 3Nadreen OsmanNo ratings yet
- Adhf 2023Document25 pagesAdhf 2023Mahamed Wefkey OmranNo ratings yet
- Acute Coronary SyndrommeDocument50 pagesAcute Coronary SyndrommeAndriani Kemala SariNo ratings yet
- Anaesthesia For TURPDocument6 pagesAnaesthesia For TURPMutia FarinaNo ratings yet
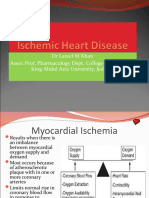
- Ischemic Heart Diease PDFDocument33 pagesIschemic Heart Diease PDFMahamed Wefkey OmranNo ratings yet
- BSC Summary 2019 ESC Guidelines PDFDocument11 pagesBSC Summary 2019 ESC Guidelines PDFNick StamatiadisNo ratings yet
- Acute Coronary Syndrome Pathophysiology & TreatmentDocument18 pagesAcute Coronary Syndrome Pathophysiology & TreatmentLillian KrazemNo ratings yet
- Brain Attack by Dr. RABEE ALANSI SANAA YEMENDocument31 pagesBrain Attack by Dr. RABEE ALANSI SANAA YEMENdrrabe3No ratings yet
- Chest: Antithrombotic and Thrombolytic Therapy For Valvular DiseaseDocument25 pagesChest: Antithrombotic and Thrombolytic Therapy For Valvular DiseaseIvan FirmansyahNo ratings yet
- Assign 1 - Cardiovascular System - ANSWER KEYDocument6 pagesAssign 1 - Cardiovascular System - ANSWER KEYF6imNo ratings yet
- All Past Rounds Cardio MCQs AlexandriaDocument37 pagesAll Past Rounds Cardio MCQs AlexandriaMahmoud Abouelsoud100% (1)
- RANASINGHE Cardiac Function & Disease & AnesthesiaDocument51 pagesRANASINGHE Cardiac Function & Disease & AnesthesiaDagimNo ratings yet
- CHAPTER 56 - Unstable Angina and Non-ST ElevationDocument34 pagesCHAPTER 56 - Unstable Angina and Non-ST ElevationSatria WardanaNo ratings yet
- Antithrombotic Dilemmas in Stroke MedicineDocument43 pagesAntithrombotic Dilemmas in Stroke MedicineGopi Krishnan RNo ratings yet
- ACC/AHA STEMI GuidelinesDocument94 pagesACC/AHA STEMI GuidelinesDika DekokNo ratings yet
- Stroke Prevention and Management Guideline SummaryDocument24 pagesStroke Prevention and Management Guideline Summarynisha24100% (1)
- CARDIOLOGY TIPSDocument53 pagesCARDIOLOGY TIPSPangalanitaNo ratings yet
- Chapter 28 Management of Patients With StructuralDocument23 pagesChapter 28 Management of Patients With StructuralAbel C. Idusma Jr.No ratings yet
- Ischemic Heart Disease Revised LMKDocument50 pagesIschemic Heart Disease Revised LMKLateef KhanNo ratings yet
- Cardiogenic ShockDocument42 pagesCardiogenic ShockpashaNo ratings yet
- Summary 2013 Esc GuidelinesDocument8 pagesSummary 2013 Esc GuidelinesNick StamatiadisNo ratings yet
- Treatment of NSTE-ACSDocument4 pagesTreatment of NSTE-ACSAnuradha NanayakkaraNo ratings yet
- Increased frequency of advanced fibrosis in individuals with elevated iron levelsDocument2 pagesIncreased frequency of advanced fibrosis in individuals with elevated iron levelsalinna1980No ratings yet
- 1.1.1 European Society of Cardiology (ESC) : GuidelinesDocument3 pages1.1.1 European Society of Cardiology (ESC) : GuidelinesMhmad MayhobNo ratings yet
- Coronary Artery Bypass Graft SurgeryDocument8 pagesCoronary Artery Bypass Graft SurgeryJatin SinghNo ratings yet
- Medical Management of Rheumatic Heart DiseaseDocument23 pagesMedical Management of Rheumatic Heart DiseaseirineNo ratings yet
- 2019 BR C QuestionsDocument369 pages2019 BR C Questionsmanoj kumarNo ratings yet
- CPG 2011 - Unstable Angine and NSTEMI.Document62 pagesCPG 2011 - Unstable Angine and NSTEMI.drnado_82No ratings yet
- 2014 Changes in NSTE-ACSDocument4 pages2014 Changes in NSTE-ACSnbnbNo ratings yet
- KillipsDocument12 pagesKillipsNhorlyn Adante SoltesNo ratings yet
- CARDIOLOGY 22/05/21: Dian Paramita Kartikasari, DR., SP - JPDocument58 pagesCARDIOLOGY 22/05/21: Dian Paramita Kartikasari, DR., SP - JPDian ParamitaNo ratings yet
- MCQ Cardio 1Document64 pagesMCQ Cardio 1Dian Paramita0% (1)
- Cardiolog Y: Dian Paramita Kartikasari MAY, 17THDocument51 pagesCardiolog Y: Dian Paramita Kartikasari MAY, 17THDian ParamitaNo ratings yet
- D. ST Elevations in Lead V4RDocument4 pagesD. ST Elevations in Lead V4RDian ParamitaNo ratings yet
- Antihypertensive Agents that Reduce Uric Acid and Migraines or Cause GynecomastiaDocument53 pagesAntihypertensive Agents that Reduce Uric Acid and Migraines or Cause GynecomastiaDian ParamitaNo ratings yet
- MCQ Cardio 1Document64 pagesMCQ Cardio 1Dian Paramita0% (1)
- MCQ Cardio 3Document50 pagesMCQ Cardio 3Dian ParamitaNo ratings yet
- MCQ Cardio 2Document54 pagesMCQ Cardio 2Dian Paramita100% (1)
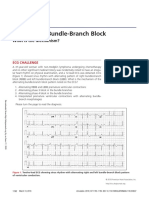
- Alternating Bundle-Branch Block: CirculationDocument3 pagesAlternating Bundle-Branch Block: CirculationDian ParamitaNo ratings yet
- QT interval drugs ECG chest painDocument7 pagesQT interval drugs ECG chest painDian ParamitaNo ratings yet
- Cdi2012 820827Document9 pagesCdi2012 820827Dian ParamitaNo ratings yet
- Chistiakov 2016Document58 pagesChistiakov 2016Dian ParamitaNo ratings yet
- Al Hasani2019Document22 pagesAl Hasani2019Dian ParamitaNo ratings yet
- Iocl Section 1 - Process SpecficationDocument73 pagesIocl Section 1 - Process SpecficationYogi173No ratings yet
- 18 National Indicator Framework For Monitoring Evaluation Myanmar Ye Naing HtetDocument9 pages18 National Indicator Framework For Monitoring Evaluation Myanmar Ye Naing HtetKo KyawNo ratings yet
- Welfare Schemes in TelanganaDocument46 pagesWelfare Schemes in TelanganaNare ChallagondlaNo ratings yet
- Slide BP Texas City RefineryDocument20 pagesSlide BP Texas City Refineryamaleena_muniraNo ratings yet
- PT. Citilink Indonesia N P W P: 0 2 - 8 2 7 - 5 9 7 - 2 - 0 9 3 - 0 0 0 Jl. Raya Juanda Sawotratap Gedangan SidoarjoDocument2 pagesPT. Citilink Indonesia N P W P: 0 2 - 8 2 7 - 5 9 7 - 2 - 0 9 3 - 0 0 0 Jl. Raya Juanda Sawotratap Gedangan SidoarjoZemNo ratings yet
- Physical ExaminationDocument7 pagesPhysical ExaminationCha CulveraNo ratings yet
- Standardized Recipes - Doc2Document130 pagesStandardized Recipes - Doc2epic failNo ratings yet
- EVBAT00100 Batterij ModuleDocument1 pageEVBAT00100 Batterij ModuleSaptCahbaguzNo ratings yet
- Practical-2 Simulation of ReactorsDocument2 pagesPractical-2 Simulation of ReactorsniralNo ratings yet
- Marketing Environment Analysis and Trends Impacting CompaniesDocument27 pagesMarketing Environment Analysis and Trends Impacting CompaniesSamoyed KalraNo ratings yet
- 可汗语法48篇(明志教育推荐) PDFDocument163 pages可汗语法48篇(明志教育推荐) PDFtellmewhour100% (2)
- Space suit essentialsDocument6 pagesSpace suit essentialsAdam PaiggeNo ratings yet
- 7Document40 pages7Felipe RichardiosNo ratings yet
- Exe Summ RajatCement Eng PDFDocument12 pagesExe Summ RajatCement Eng PDFflytorahulNo ratings yet
- Piston Water MeterDocument2 pagesPiston Water MeterMark PamularNo ratings yet
- Research 1Document7 pagesResearch 1Rhea Mae ObligarNo ratings yet
- Klubermatic Lubricant DispensersDocument13 pagesKlubermatic Lubricant Dispenserstatankise100% (1)
- ResiboDocument1 pageResiboAlex RespicioNo ratings yet
- Thematic Apperception TestDocument127 pagesThematic Apperception TestRitu yousufNo ratings yet
- Fy em - 1 Question Bank 2023-24Document9 pagesFy em - 1 Question Bank 2023-24raju.sharmqNo ratings yet
- RA 6541 National Building Code of The PH StandPipeDocument5 pagesRA 6541 National Building Code of The PH StandPipejungzki jungzkiNo ratings yet
- Hedging FuturesDocument39 pagesHedging Futuresapi-3833893100% (1)
- On of Smart Crab Water Monitoring System Using ArduinoDocument46 pagesOn of Smart Crab Water Monitoring System Using ArduinoLayla GarciaNo ratings yet
- Bonding BB1Document3 pagesBonding BB1DeveshNo ratings yet
- Pipe Material & Dimension Standard MatrixDocument2 pagesPipe Material & Dimension Standard MatrixHemantNo ratings yet
- NABARD Presentation On FPODocument14 pagesNABARD Presentation On FPOSomnath DasGupta71% (7)
- Kami Export - Jervocus Aiken - Ecosystem Project TEMPLATE 2023Document7 pagesKami Export - Jervocus Aiken - Ecosystem Project TEMPLATE 2023Jervocus AikenNo ratings yet
- Cavab - kartı - numune (копия) (копия) (копия) (копия)Document2 pagesCavab - kartı - numune (копия) (копия) (копия) (копия)Javid NovruzovNo ratings yet
- Application Format For Child CustodyDocument2 pagesApplication Format For Child CustodyDHUP CHAND JAISWAL100% (3)
- Plastipak PresentationDocument28 pagesPlastipak Presentationapi-608970005No ratings yet