You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Wiring Diagram Elevator: PT - Industri Lift Indo NusantaraDocument28 pagesWiring Diagram Elevator: PT - Industri Lift Indo NusantaraGogik AntoNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Corrosion Protection With Eco-Friendly InhibitorsDocument7 pagesCorrosion Protection With Eco-Friendly InhibitorsPeterNo ratings yet
- (Wiki) Battle of The Korsun-Cherkassy PocketDocument12 pages(Wiki) Battle of The Korsun-Cherkassy PocketAndrea MatteuzziNo ratings yet
- Sitagliptin Slide Set Specialist - 1Document31 pagesSitagliptin Slide Set Specialist - 1Fannia Setiani100% (1)
- 1st Term Revision Sheet Primary 6Document38 pages1st Term Revision Sheet Primary 6Mark AdelNo ratings yet
- Sika Waterbar® - PVC-P NB Type D: Product Data SheetDocument4 pagesSika Waterbar® - PVC-P NB Type D: Product Data SheetKhin Sandi KoNo ratings yet
- I7 2011Document70 pagesI7 2011Dorin SimioanaNo ratings yet
- A K Ramanujan Says About The River Vaikai in This PoemDocument3 pagesA K Ramanujan Says About The River Vaikai in This Poemsarayoo100% (1)
- Pancreas Function: Acute PancreatitisDocument2 pagesPancreas Function: Acute PancreatitisMemory MahwendaNo ratings yet
- PHILIPS CH - LC7.1HE LA PDFDocument91 pagesPHILIPS CH - LC7.1HE LA PDFnik3654No ratings yet
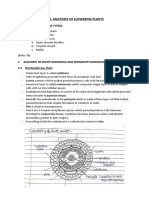
- CH6 - Anatomy of Flowering Plants - NotesDocument4 pagesCH6 - Anatomy of Flowering Plants - NotesanuminiatureNo ratings yet
- Weir 1984Document12 pagesWeir 1984IcsNo ratings yet
- Customer Relationship Management: Nestle)Document18 pagesCustomer Relationship Management: Nestle)Nitin KherajmalaniNo ratings yet
- Data Word Bank-1Document868 pagesData Word Bank-1Park Ilmaa KimNo ratings yet
- Section 4.6Document3 pagesSection 4.6Chang BrootNo ratings yet
- Navara - RiceDocument3 pagesNavara - RiceRavi ShankarNo ratings yet
- 12r-Asia Enterprise Comet PricelistDocument1 page12r-Asia Enterprise Comet PricelistBong PelotinNo ratings yet
- Formulir Review Judul Skripsi 2019 (Update 28 Maret 2019) Kevin ThenediDocument2 pagesFormulir Review Judul Skripsi 2019 (Update 28 Maret 2019) Kevin ThenediKevin ThenediNo ratings yet
- Infra-Red CAR-KEY Transmitter: OM1058 in Case SO-8Document4 pagesInfra-Red CAR-KEY Transmitter: OM1058 in Case SO-8José SilvaNo ratings yet
- Billprint 16030727Document1 pageBillprint 16030727Ruloans VaishaliNo ratings yet
- Wide Belt Sanding Machines SANDTEQ W 300 700 en PDFDocument48 pagesWide Belt Sanding Machines SANDTEQ W 300 700 en PDFMesara Kod KokijaNo ratings yet
- 5608-Article Text-20048-1-10-20210319Document4 pages5608-Article Text-20048-1-10-20210319Muhammad IzehagaNo ratings yet
- A Simplified Finite Element Model For Structural Cable Bending MechanismDocument15 pagesA Simplified Finite Element Model For Structural Cable Bending MechanismJoaquin VieraNo ratings yet
- Industrial Report FinalDocument118 pagesIndustrial Report FinalArahvinth Obula KrishnamoorthyNo ratings yet
- A Visit From ST NickDocument2 pagesA Visit From ST NickJohn BarefieldNo ratings yet
- Agroforestry Primer 01Document10 pagesAgroforestry Primer 01vjvarNo ratings yet
- Case Study: Tourism and Biodiversity (Ecotourism - A Sustainable Development Tool, A Case For Belize)Document34 pagesCase Study: Tourism and Biodiversity (Ecotourism - A Sustainable Development Tool, A Case For Belize)Aarthi PadmanabhanNo ratings yet
- SLESDocument5 pagesSLESAllyana TiemsimNo ratings yet
- Course Learning Outcome (CLO), Delivery and Assessment TemplateDocument2 pagesCourse Learning Outcome (CLO), Delivery and Assessment TemplateAbu MuhammadNo ratings yet
- Verus CFT CommercialDocument2 pagesVerus CFT CommercialLuchin SheckNo ratings yet