You might also like
- Eating Disorders: DR Jibril Handuleh Amoud UniversityDocument11 pagesEating Disorders: DR Jibril Handuleh Amoud UniversityOmar AbdillahiNo ratings yet
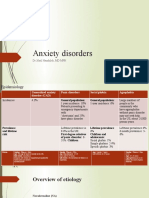
- Anxiety Disorders: DR Jibril Handuleh, MD MPHDocument39 pagesAnxiety Disorders: DR Jibril Handuleh, MD MPHOmar AbdillahiNo ratings yet
- Psychiatry CourseDocument29 pagesPsychiatry CourseOmar AbdillahiNo ratings yet
- Mood Disorders: DR Jibril Handuleh Amoud UniversityDocument73 pagesMood Disorders: DR Jibril Handuleh Amoud UniversityOmar AbdillahiNo ratings yet
- Psychiatric Signs and SymptomsDocument19 pagesPsychiatric Signs and SymptomsOmar Abdillahi100% (1)
- Hypertensive Emergency: Group ThreeDocument11 pagesHypertensive Emergency: Group ThreeOmar AbdillahiNo ratings yet
- ENDO... ElectrolyteDocument44 pagesENDO... ElectrolyteOmar AbdillahiNo ratings yet
- Approach To Abdominal PainDocument22 pagesApproach To Abdominal PainOmar AbdillahiNo ratings yet
- Diabetic Ketoacidosis (DKA) and Hyperosmolar Hyperglycemic State (HHS)Document25 pagesDiabetic Ketoacidosis (DKA) and Hyperosmolar Hyperglycemic State (HHS)Omar Abdillahi100% (1)
- DVT and PeDocument25 pagesDVT and PeOmar AbdillahiNo ratings yet
- Chronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredDocument25 pagesChronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredOmar AbdillahiNo ratings yet
- Acute Kidney Injury (AKI)Document50 pagesAcute Kidney Injury (AKI)Omar AbdillahiNo ratings yet
- DVT and PeDocument25 pagesDVT and PeOmar AbdillahiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Movie Billy Elliot Questions: Read and Answer The Questions, Choose The Correct One According To The MovieDocument1 pageMovie Billy Elliot Questions: Read and Answer The Questions, Choose The Correct One According To The MovieAlejandro FuentesNo ratings yet
- Ace Magashule Challenges High Court Loss in Supreme CourtDocument14 pagesAce Magashule Challenges High Court Loss in Supreme CourtjillianNo ratings yet
- Samplex MidtermsDocument10 pagesSamplex Midtermsnichols greenNo ratings yet
- Daftar Hadir Mahasiswa PPKN A Matkul Filsafat PancasilaDocument2 pagesDaftar Hadir Mahasiswa PPKN A Matkul Filsafat Pancasilamuja hidinNo ratings yet
- Analysis PaperDocument9 pagesAnalysis PaperSean Gementiza CabalseNo ratings yet
- Sachika & Ketan Torts Sem II NotesDocument54 pagesSachika & Ketan Torts Sem II NotesYash solankiNo ratings yet
- Quick Placement TestDocument11 pagesQuick Placement TestLCARDILES6337No ratings yet
- The Chiong Sisters Murder CaseDocument5 pagesThe Chiong Sisters Murder CaseMarie Joice PandanNo ratings yet
- People v. Lagman, G.R. No. L-45892, & People v. Zosa, G.R. No. L-45893Document1 pagePeople v. Lagman, G.R. No. L-45892, & People v. Zosa, G.R. No. L-45893Daryl CruzNo ratings yet
- Lea 101 ModuleDocument30 pagesLea 101 ModuleEchardeen Reeka Camilan MillendezNo ratings yet
- MARIAN Rewrite The Following Sentences Using The Correct Conditional ClauseDocument2 pagesMARIAN Rewrite The Following Sentences Using The Correct Conditional ClauseElena Martín0% (1)
- The Glorious Destination of An Ummah (English)Document19 pagesThe Glorious Destination of An Ummah (English)Dar Haqq (Ahl'al-Sunnah Wa'l-Jama'ah)No ratings yet
- Evangelista v. People G.R. No. 163267 May 5 2010Document2 pagesEvangelista v. People G.R. No. 163267 May 5 2010Kyla Ellen CalelaoNo ratings yet
- HHRG 116 VR09 Bio SiedorM 20200708Document11 pagesHHRG 116 VR09 Bio SiedorM 20200708Kristopher KrodyNo ratings yet
- Shivangi Digant ShahDocument10 pagesShivangi Digant ShahSabari Nathan MariappanNo ratings yet
- 1) Letter Request To Terminate Fuel Supply and Equipment Loan AgreementDocument1 page1) Letter Request To Terminate Fuel Supply and Equipment Loan AgreementDavao LegalNo ratings yet
- Chapter 7 The SouthlandDocument6 pagesChapter 7 The SouthlandJose RodriguezNo ratings yet
- Suspense - Types - 1Document7 pagesSuspense - Types - 1Екатерина МитюковаNo ratings yet
- CHAPTER 6, 7,8,9 Classes of Defective Contracts (JURADO)Document3 pagesCHAPTER 6, 7,8,9 Classes of Defective Contracts (JURADO)LawStudent101412No ratings yet
- Undang2 Versi Ku Din Ku MehDocument19 pagesUndang2 Versi Ku Din Ku MehLatifah AtirahNo ratings yet
- 2-Perez vs. Medical CityDocument8 pages2-Perez vs. Medical CityFatzie MendozaNo ratings yet
- Diss-Module 12-13Document10 pagesDiss-Module 12-13Eleazar De TorresNo ratings yet
- Spontanous Pneumothorax, Pulmonary Cysts, Blebs, BullaeDocument47 pagesSpontanous Pneumothorax, Pulmonary Cysts, Blebs, BullaedhabeNo ratings yet
- Elise Lemire - Miscegenation - Making Race in America-University of Pennsylvania Press (2009)Document215 pagesElise Lemire - Miscegenation - Making Race in America-University of Pennsylvania Press (2009)Maurizio80No ratings yet
- Substitution of PartiesDocument4 pagesSubstitution of PartiesHarold MapeNo ratings yet
- Chapter Bylaws of The Classical Academy High School Chapter of The National Honor Society Adopted: On This Day, 6th of December in The Year 2016Document7 pagesChapter Bylaws of The Classical Academy High School Chapter of The National Honor Society Adopted: On This Day, 6th of December in The Year 2016api-337440242No ratings yet
- Aaron JADocument5 pagesAaron JAAaron ReyesNo ratings yet
- Lesson 4 Final Income Taxation PDFDocument4 pagesLesson 4 Final Income Taxation PDFErika ApitaNo ratings yet
- To Kill A MockingbirdDocument10 pagesTo Kill A MockingbirdAdeel MalikNo ratings yet