You might also like
- Mood Disorders: Major Depressive DisorderDocument15 pagesMood Disorders: Major Depressive DisorderJacecosmozNo ratings yet
- An Assessment of Five (PANSS, SAPS, SANS, NSA-16, CGI-SCH) CommonlyDocument7 pagesAn Assessment of Five (PANSS, SAPS, SANS, NSA-16, CGI-SCH) Commonlysyarifah husna100% (1)
- A Case Study of Generalized Anxiety DisorderDocument10 pagesA Case Study of Generalized Anxiety DisorderRina PerezNo ratings yet
- Clinical Global Impression-Bipolar (Cgi-Bp)Document2 pagesClinical Global Impression-Bipolar (Cgi-Bp)abhilasha8dwivediNo ratings yet
- SchizophreniaDocument2 pagesSchizophreniaIT’S ME HAYLA100% (1)
- Physical and Mental Disability TestDocument9 pagesPhysical and Mental Disability TestANITTA SNo ratings yet
- Mental Status ExaminationDocument7 pagesMental Status ExaminationChristine MatasNo ratings yet
- Panss ScoreDocument8 pagesPanss ScoretriaclaresiaNo ratings yet
- 04 - ADHD Diagnosis and Testing Guide - ADD Symptom EvaluationsDocument7 pages04 - ADHD Diagnosis and Testing Guide - ADD Symptom EvaluationstenahernanNo ratings yet
- Schizophrenia: Causes, Incidence, and Risk FactorsDocument3 pagesSchizophrenia: Causes, Incidence, and Risk FactorsNurul Hidayah IbrahimNo ratings yet
- Case History FormatDocument7 pagesCase History FormatSaranya R VNo ratings yet
- Young's Schema Questionnaire - Short Form Version 3 (YSQ-S3) : Preliminary Validation in Older AdultsDocument35 pagesYoung's Schema Questionnaire - Short Form Version 3 (YSQ-S3) : Preliminary Validation in Older AdultsFiona DayNo ratings yet
- Management of Childhood and Adolescent DisordersDocument26 pagesManagement of Childhood and Adolescent Disordersdurgesh yadav100% (1)
- Rle Case Study 5Document12 pagesRle Case Study 5Angel May P AgotNo ratings yet
- Bernard Gallagher Cap. 5 Sociology of Mental IllnessDocument16 pagesBernard Gallagher Cap. 5 Sociology of Mental IllnessLaura CristinaNo ratings yet
- Final ThesisDocument120 pagesFinal ThesisSingh SoniyaNo ratings yet
- Validity R:: All Descriptive Statistics Presented in This Handout Are For An Adult Nonpatient Population (Table 1)Document40 pagesValidity R:: All Descriptive Statistics Presented in This Handout Are For An Adult Nonpatient Population (Table 1)Marina SwansonNo ratings yet
- Understanding Generalized Anxiety DisorderDocument9 pagesUnderstanding Generalized Anxiety Disorderselina shakyaNo ratings yet
- The Influence of Special Psychological Training (Attention, Focusing) On Supes Students in Achieving Sports Performance in Table TennisDocument8 pagesThe Influence of Special Psychological Training (Attention, Focusing) On Supes Students in Achieving Sports Performance in Table TennisArsene IgorNo ratings yet
- Psych Case StudyDocument14 pagesPsych Case StudySmridhi Seth100% (1)
- Interpersonal Emotion Regulation Questionnaire (IERQ) : Scale Development and Psychometric CharacteristicsDocument16 pagesInterpersonal Emotion Regulation Questionnaire (IERQ) : Scale Development and Psychometric CharacteristicsDario CornejoNo ratings yet
- Burnout-Depression Overlap - A ReviewDocument15 pagesBurnout-Depression Overlap - A ReviewMarcelo PinheiroNo ratings yet
- Neurobiology of Anxiety Disorders: Michael J. Meaney, Michael R. Liebowitz, and E. David LeonardoDocument43 pagesNeurobiology of Anxiety Disorders: Michael J. Meaney, Michael R. Liebowitz, and E. David LeonardoOscar René Hernández PérezNo ratings yet
- Characteristics of Clinical PsychologistDocument6 pagesCharacteristics of Clinical PsychologistMahnoor MalikNo ratings yet
- Adjustment Disorders in Dsm5 Implications For Occupationalhealth SurveillanceDocument4 pagesAdjustment Disorders in Dsm5 Implications For Occupationalhealth SurveillancealinaneagoeNo ratings yet
- Clinical Conference Case Study Family ViolenceDocument1 pageClinical Conference Case Study Family ViolenceIvy LaNo ratings yet
- Oxford Handbooks Online: Intellectual DisabilitiesDocument20 pagesOxford Handbooks Online: Intellectual DisabilitiesCristina100% (1)
- Guilford Press FlyerDocument2 pagesGuilford Press FlyerskkundorNo ratings yet
- MADRSDocument6 pagesMADRSorestis_baNo ratings yet
- Psychiatry Info - FinalDocument8 pagesPsychiatry Info - FinalH_QasimNo ratings yet
- Course of OCDDocument16 pagesCourse of OCDShwetank BansalNo ratings yet
- Week 2 (OSCE CASC Book II 2018-19) 03.09.2018Document48 pagesWeek 2 (OSCE CASC Book II 2018-19) 03.09.2018Andrew WdsmithNo ratings yet
- 21.cpsy.034 Icd-10&dsm-5Document8 pages21.cpsy.034 Icd-10&dsm-5Victor YanafNo ratings yet
- The Investigation and Differential Diagnosis of Asperger Syndrome in AdultsDocument9 pagesThe Investigation and Differential Diagnosis of Asperger Syndrome in AdultsamarillonoexpectaNo ratings yet
- Raven's Coloured Progressive Matrices Test Norms for Omani ChildrenDocument15 pagesRaven's Coloured Progressive Matrices Test Norms for Omani ChildrenCH KarimNo ratings yet
- Rating Scales for Assessing Bipolar Disorder SymptomsDocument14 pagesRating Scales for Assessing Bipolar Disorder SymptomsDivia RainaNo ratings yet
- Comparison Bet ICD & DSM PDFDocument18 pagesComparison Bet ICD & DSM PDFTiffany SyNo ratings yet
- Shalit - Efficiency of PsychotherapyDocument9 pagesShalit - Efficiency of PsychotherapyAyerevNo ratings yet
- Neopir CaietDocument9 pagesNeopir CaietAncaNo ratings yet
- Guide to Treating DeliriumDocument14 pagesGuide to Treating DeliriumSendruc OvidiuNo ratings yet
- Handouts YBOC Symptom ChecklistDocument2 pagesHandouts YBOC Symptom ChecklistJoem cNo ratings yet
- DPC Field Report CompletedDocument36 pagesDPC Field Report Completedraman_bhoomi9910No ratings yet
- Child Psychiatry History Clerking Sheet-1Document3 pagesChild Psychiatry History Clerking Sheet-1khairiah09No ratings yet
- Psychodiagnostics and Psychological AssessmentDocument4 pagesPsychodiagnostics and Psychological AssessmentBim arra0% (1)
- Screening BDDQ PDFDocument37 pagesScreening BDDQ PDFManuelaMartinezNo ratings yet
- Psychiatric Diagnosis: Challenges and ProspectsFrom EverandPsychiatric Diagnosis: Challenges and ProspectsIhsan M. SalloumRating: 5 out of 5 stars5/5 (1)
- Good Touch-Bad TouchDocument22 pagesGood Touch-Bad Touchyogesh_funde100% (1)
- Introduction To The Types of Mental IllnessesDocument23 pagesIntroduction To The Types of Mental IllnessesCathy-Ann Carby100% (1)
- Module 3 Biochemistry of The BrainDocument12 pagesModule 3 Biochemistry of The BrainSakshi Jauhari100% (1)
- CDI Patient VersionDocument9 pagesCDI Patient VersionalotfyaNo ratings yet
- SNAP-IV-C Rating Scale: Test For Attention, Hyperactivity and ImpulsivityDocument1 pageSNAP-IV-C Rating Scale: Test For Attention, Hyperactivity and ImpulsivityHemant KumarNo ratings yet
- The Clinical Assessment Interview For Negative SymDocument9 pagesThe Clinical Assessment Interview For Negative SymJohanes DavidNo ratings yet
- APA - DSM 5 Diagnoses For Children PDFDocument3 pagesAPA - DSM 5 Diagnoses For Children PDFharis pratamsNo ratings yet
- Negative Symptoms EQZ Lancet ReviewDocument14 pagesNegative Symptoms EQZ Lancet ReviewConstanza González GutiérrezNo ratings yet
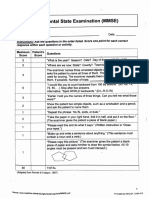
- Mini-Mental State Examination (MMSE)Document3 pagesMini-Mental State Examination (MMSE)Prescilla San PedroNo ratings yet
- Test Personal It AteDocument9 pagesTest Personal It AteMihaela Sindie0% (1)
- An Update On The Comorbidity of ADHD and ASDDocument16 pagesAn Update On The Comorbidity of ADHD and ASDCristina SolerNo ratings yet
- Causes and Risk Factors For Attention-Deficit Hyperactivity DisorderDocument8 pagesCauses and Risk Factors For Attention-Deficit Hyperactivity DisorderFranthesa LayloNo ratings yet
- Cultural Adaptation of CBT for Serious Mental Illness: A Guide for Training and PracticeFrom EverandCultural Adaptation of CBT for Serious Mental Illness: A Guide for Training and PracticeNo ratings yet
- Teenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenFrom EverandTeenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenNo ratings yet
- Eating Disorders: DR Jibril Handuleh Amoud UniversityDocument11 pagesEating Disorders: DR Jibril Handuleh Amoud UniversityOmar AbdillahiNo ratings yet
- Suicide and Self-HarmDocument32 pagesSuicide and Self-HarmOmar AbdillahiNo ratings yet
- Psychiatry CourseDocument29 pagesPsychiatry CourseOmar AbdillahiNo ratings yet
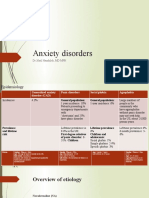
- Anxiety Disorders: DR Jibril Handuleh, MD MPHDocument39 pagesAnxiety Disorders: DR Jibril Handuleh, MD MPHOmar AbdillahiNo ratings yet
- Psychiatry CourseDocument29 pagesPsychiatry CourseOmar AbdillahiNo ratings yet
- PneumothoraxDocument26 pagesPneumothoraxOmar AbdillahiNo ratings yet
- ENDO... ElectrolyteDocument44 pagesENDO... ElectrolyteOmar AbdillahiNo ratings yet
- Thyroid Emergencies: Recognition and ManagementDocument51 pagesThyroid Emergencies: Recognition and ManagementOmar AbdillahiNo ratings yet
- Psychiatric Signs and SymptomsDocument19 pagesPsychiatric Signs and SymptomsOmar Abdillahi100% (1)
- Approach To Abdominal PainDocument22 pagesApproach To Abdominal PainOmar AbdillahiNo ratings yet
- Venous Thromboembolism Disease Risks, Symptoms and TreatmentDocument25 pagesVenous Thromboembolism Disease Risks, Symptoms and TreatmentOmar AbdillahiNo ratings yet
- Hypertensive Emergency: Group ThreeDocument11 pagesHypertensive Emergency: Group ThreeOmar AbdillahiNo ratings yet
- Venous Thromboembolism Disease Risks, Symptoms and TreatmentDocument25 pagesVenous Thromboembolism Disease Risks, Symptoms and TreatmentOmar AbdillahiNo ratings yet
- Chronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredDocument25 pagesChronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredOmar AbdillahiNo ratings yet
- Diabetic Ketoacidosis (DKA) and Hyperosmolar Hyperglycemic State (HHS)Document25 pagesDiabetic Ketoacidosis (DKA) and Hyperosmolar Hyperglycemic State (HHS)Omar Abdillahi100% (1)
- Chronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredDocument25 pagesChronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredOmar AbdillahiNo ratings yet
- Diabetic Ketoacidosis (DKA) and Hyperosmolar Hyperglycemic State (HHS)Document25 pagesDiabetic Ketoacidosis (DKA) and Hyperosmolar Hyperglycemic State (HHS)Omar Abdillahi100% (1)
- Acute Kidney Injury (AKI)Document50 pagesAcute Kidney Injury (AKI)Omar AbdillahiNo ratings yet
- AsthmaDocument30 pagesAsthmaOmar AbdillahiNo ratings yet
- AsthmaDocument30 pagesAsthmaOmar AbdillahiNo ratings yet
- Individual Essay 3: BUS 314 - Organizational BehaviorDocument4 pagesIndividual Essay 3: BUS 314 - Organizational BehaviorDuyên NguyễnNo ratings yet
- Unit 3Document3 pagesUnit 3Audrina WesleyNo ratings yet
- ABC of Psychological Medicine - R. Mayou, M. Sharpe, A. CarsonDocument69 pagesABC of Psychological Medicine - R. Mayou, M. Sharpe, A. CarsonstuarttudorNo ratings yet
- Research TopicsDocument2 pagesResearch TopicsClareen JuneNo ratings yet
- Physical and Mental Changes in AdolescenceDocument18 pagesPhysical and Mental Changes in AdolescenceThâlíä Oç Mó100% (1)
- Trauma Informed Coping Skills PDFDocument45 pagesTrauma Informed Coping Skills PDFYong Chen100% (3)
- Chapter 6 - Perception & Individual Decision MakingDocument29 pagesChapter 6 - Perception & Individual Decision MakingEshnat Mumtahina MridhaNo ratings yet
- NCP For Pre-Op Incision CaseDocument8 pagesNCP For Pre-Op Incision CaseFAt TyNo ratings yet
- Career - Development - Theories - Super'sDocument15 pagesCareer - Development - Theories - Super'sEl Comedor BenedictNo ratings yet
- Kleptomania and HomoeopathyDocument7 pagesKleptomania and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Duke University Religion IndexDocument1 pageDuke University Religion IndexSubas BiswasNo ratings yet
- Avoidant Personality DisorderDocument1 pageAvoidant Personality DisorderDylan LiuNo ratings yet
- Human Performance Limitations and the SHEL ModelDocument8 pagesHuman Performance Limitations and the SHEL ModelChan Sin Loon80% (10)
- Theoretical Foundations of Nursing / Nursing Care ManagementDocument16 pagesTheoretical Foundations of Nursing / Nursing Care ManagementJhae Zharie Delasan PanosoNo ratings yet
- Passion for Special Education MastersDocument2 pagesPassion for Special Education MasterstptmNo ratings yet
- 19 Perceptions PDFDocument6 pages19 Perceptions PDFIJELS Research JournalNo ratings yet
- Manan Prakashan 1Document8 pagesManan Prakashan 1Raj jadhavNo ratings yet
- WHO International Bibliography of KMCDocument84 pagesWHO International Bibliography of KMCSapna thakurNo ratings yet
- Theories of Emotion in PsychologyDocument1 pageTheories of Emotion in PsychologyRj BengilNo ratings yet
- Personality and Individual Differences: Umit Akirmak, Pinar AylaDocument5 pagesPersonality and Individual Differences: Umit Akirmak, Pinar Aylavivi nauraNo ratings yet
- HR Interview QuestionDocument74 pagesHR Interview QuestionManmohan SahuNo ratings yet
- Leadership Styles ExplainedDocument8 pagesLeadership Styles Explainedbiodun oNo ratings yet
- Emotionnal Intelligence NDocument26 pagesEmotionnal Intelligence Nrabin neupaneNo ratings yet
- Solo Sex BehaviorDocument35 pagesSolo Sex BehaviordrnyolNo ratings yet
- Dwight Shrute Mental Disorder FunnyDocument5 pagesDwight Shrute Mental Disorder FunnyReesie ZahnerNo ratings yet
- Abu BakerDocument19 pagesAbu Bakerramakrishn34aananthaNo ratings yet
- Mapeh: Sports OfficiatingDocument9 pagesMapeh: Sports OfficiatingRafael De VeraNo ratings yet
- Narrqative Report 2Document6 pagesNarrqative Report 2Christine CelestiNo ratings yet
- Love, Intimacy, and RelationshipDocument17 pagesLove, Intimacy, and RelationshipLovely Grace Cajegas100% (1)
- Difference Between Personnel Management and Human Resource ManagementDocument18 pagesDifference Between Personnel Management and Human Resource ManagementLoueljie Antigua100% (1)