You might also like
- Raven's Coloured Progressive Matrices Test Norms for Omani ChildrenDocument15 pagesRaven's Coloured Progressive Matrices Test Norms for Omani ChildrenCH KarimNo ratings yet
- The Autism Observation Scale For Infants: Scale Development and Reliability DataDocument8 pagesThe Autism Observation Scale For Infants: Scale Development and Reliability DataRenata de Mesquita Ferraz LucenaNo ratings yet
- Behavior Therapy: DR Saima MajeedDocument33 pagesBehavior Therapy: DR Saima MajeedUkhtSameehNo ratings yet
- Schizophrenia: Causes, Incidence, and Risk FactorsDocument3 pagesSchizophrenia: Causes, Incidence, and Risk FactorsNurul Hidayah IbrahimNo ratings yet
- Handouts YBOC Symptom ChecklistDocument2 pagesHandouts YBOC Symptom ChecklistJoem cNo ratings yet
- BKT NotesDocument6 pagesBKT NotesPallavi ChopraNo ratings yet
- Five Factor Model of Personality, Assessment ofDocument6 pagesFive Factor Model of Personality, Assessment ofGECJNo ratings yet
- CGASDocument4 pagesCGASDinny Atin AmanahNo ratings yet
- JoDD 17-1 26-37 Schroeder Et AlDocument12 pagesJoDD 17-1 26-37 Schroeder Et AlEspíritu CiudadanoNo ratings yet
- 16PF BibDocument10 pages16PF BibdocagunsNo ratings yet
- Validity study finds STAI distinguishes state and trait anxietyDocument5 pagesValidity study finds STAI distinguishes state and trait anxietyYilin NgNo ratings yet
- Physiological and psychological precursors to developing a fear of heightsDocument8 pagesPhysiological and psychological precursors to developing a fear of heightsCherry Pie Abenes CammayoNo ratings yet
- Comparison of Self-Report and Overt-Behavioral Procedures For Assessing AcrophobiaDocument7 pagesComparison of Self-Report and Overt-Behavioral Procedures For Assessing AcrophobiaMiztaloges86No ratings yet
- Children and War Foundation The Children'S Impact of Event Scale (13) CRIES-13Document5 pagesChildren and War Foundation The Children'S Impact of Event Scale (13) CRIES-13Sarah GracyntiaNo ratings yet
- Chapter 5 Powerpoint With Extra SlidesDocument111 pagesChapter 5 Powerpoint With Extra Slidesmonster40lbsNo ratings yet
- Management of Childhood and Adolescent DisordersDocument26 pagesManagement of Childhood and Adolescent Disordersdurgesh yadav100% (1)
- Conduct Disorder Fact Sheet - K. Elise Parker PDFDocument2 pagesConduct Disorder Fact Sheet - K. Elise Parker PDFepaka02No ratings yet
- OARS Adl IadlDocument5 pagesOARS Adl IadlSamuelNo ratings yet
- A Manual For Objective TAT ScoringDocument40 pagesA Manual For Objective TAT ScoringJaveriaNo ratings yet
- Case History FormatDocument7 pagesCase History FormatSaranya R VNo ratings yet
- Generic Questionnaires in Assessment of Quality of LifeDocument17 pagesGeneric Questionnaires in Assessment of Quality of LifeachyutNo ratings yet
- Assessment ReportDocument8 pagesAssessment Reportapi-359339664No ratings yet
- Oxford Handbooks Online: Intellectual DisabilitiesDocument20 pagesOxford Handbooks Online: Intellectual DisabilitiesCristina100% (1)
- Down's Syndrome Pada KehamilanDocument35 pagesDown's Syndrome Pada KehamilanArga AdityaNo ratings yet
- Validity R:: All Descriptive Statistics Presented in This Handout Are For An Adult Nonpatient Population (Table 1)Document40 pagesValidity R:: All Descriptive Statistics Presented in This Handout Are For An Adult Nonpatient Population (Table 1)Marina SwansonNo ratings yet
- Emotional Intelligence and The Trait Meta-Mood ScaleDocument13 pagesEmotional Intelligence and The Trait Meta-Mood Scalediego polinarioNo ratings yet
- PSY 3410 Autism Spectrum Disorders & Intellectual DisabilityDocument33 pagesPSY 3410 Autism Spectrum Disorders & Intellectual Disabilityncastro1319No ratings yet
- © 2018 The Guilford Press: Introduction To R PASDocument20 pages© 2018 The Guilford Press: Introduction To R PASJosi BeckerNo ratings yet
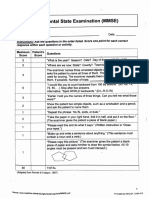
- Mini-Mental State Examination (MMSE)Document3 pagesMini-Mental State Examination (MMSE)Prescilla San PedroNo ratings yet
- Psychology AssignmentDocument7 pagesPsychology AssignmentnaveedNo ratings yet
- Differential Ability ScaleDocument26 pagesDifferential Ability ScaleHaleema BuTtNo ratings yet
- Intelligence and Emotional Disorders - PAID - 2015 PDFDocument4 pagesIntelligence and Emotional Disorders - PAID - 2015 PDFOmar Azaña Velez100% (1)
- KABC-2NU TemplateDocument3 pagesKABC-2NU TemplateLindsayNo ratings yet
- Emotional CPR - AustraliaDocument1 pageEmotional CPR - AustraliaSharon A Stocker0% (1)
- Mini Screen: P N: - D B: - D IDocument2 pagesMini Screen: P N: - D B: - D IDaniel DascaluNo ratings yet
- Subtest OriginsDocument38 pagesSubtest OriginsCharlie HultgreenNo ratings yet
- The Co-Occurrence of Intellectual Giftedness and Autism Spectrum 2011Document22 pagesThe Co-Occurrence of Intellectual Giftedness and Autism Spectrum 2011Ingrid DíazNo ratings yet
- Introduction To Approaches in Psychology Learning & Conditioning Keith ClementsDocument18 pagesIntroduction To Approaches in Psychology Learning & Conditioning Keith ClementsYunranNo ratings yet
- CV For Dr. Keely KolmesDocument9 pagesCV For Dr. Keely KolmesdrkkolmesNo ratings yet
- Group Counseling Informed Consent For ParentsDocument1 pageGroup Counseling Informed Consent For Parentsapi-239096806No ratings yet
- 2019 - Conners 3 ADHD SymptomsDocument18 pages2019 - Conners 3 ADHD Symptomsblanca_dhNo ratings yet
- Interpersonal Emotion Regulation Questionnaire (IERQ) : Scale Development and Psychometric CharacteristicsDocument16 pagesInterpersonal Emotion Regulation Questionnaire (IERQ) : Scale Development and Psychometric CharacteristicsDario CornejoNo ratings yet
- DAPT SCT HandoutDocument5 pagesDAPT SCT HandoutUdita PantNo ratings yet
- Growth and Development: Yarsi School of MedicineDocument32 pagesGrowth and Development: Yarsi School of MedicineLia Noor AnggrainiNo ratings yet
- Moral Development StagesDocument16 pagesMoral Development StagesJan Dela RosaNo ratings yet
- Neopir CaietDocument9 pagesNeopir CaietAncaNo ratings yet
- The MMSEDocument4 pagesThe MMSESiti Zubaidah HussinNo ratings yet
- Manifast Anxiety ScaleDocument14 pagesManifast Anxiety ScaleAli ArslanNo ratings yet
- NEO PIR IR Sample ReportDocument18 pagesNEO PIR IR Sample ReportBoss --No ratings yet
- Clinical Global Impression-Bipolar (Cgi-Bp)Document2 pagesClinical Global Impression-Bipolar (Cgi-Bp)abhilasha8dwivediNo ratings yet
- Assessment of Attention in PreschoolersDocument23 pagesAssessment of Attention in PreschoolersMarilda GhellereNo ratings yet
- Bip FLDocument5 pagesBip FLapi-460189664No ratings yet
- Eysenck Personality To CommunicateDocument48 pagesEysenck Personality To CommunicateYenni RoeshintaNo ratings yet
- Adaptive Behavior Assessment System-II: Technical ReportDocument5 pagesAdaptive Behavior Assessment System-II: Technical ReportLisa MariaNo ratings yet
- Dimensions ReligionDocument7 pagesDimensions ReligionArif GunawanNo ratings yet
- Negative Symptoms EQZ Lancet ReviewDocument14 pagesNegative Symptoms EQZ Lancet ReviewConstanza González GutiérrezNo ratings yet
- Rating Scales for Assessing Bipolar Disorder SymptomsDocument14 pagesRating Scales for Assessing Bipolar Disorder SymptomsDivia RainaNo ratings yet
- Theory of Mind in Normal Development and AutismDocument23 pagesTheory of Mind in Normal Development and AutismKarina CifuentesNo ratings yet
- New Directions in Interpreting the Millon Clinical Multiaxial Inventory-III (MCMI-III)From EverandNew Directions in Interpreting the Millon Clinical Multiaxial Inventory-III (MCMI-III)No ratings yet
- Study Guide to Accompany Physiological Psychology Brown/WallaceFrom EverandStudy Guide to Accompany Physiological Psychology Brown/WallaceNo ratings yet
- Social Psychology ReportDocument22 pagesSocial Psychology ReportVinyan ChinNo ratings yet
- 2020 HG Policy GuidelinesDocument29 pages2020 HG Policy GuidelinesRoderick Aspili NiervaNo ratings yet
- LET Child Development ReviewDocument25 pagesLET Child Development ReviewIrish Mendoza Seda100% (4)
- Feminism and PhilosophyDocument31 pagesFeminism and Philosophyamphi2No ratings yet
- Consumer Values, Product Benefits and Customer Value A Consumption BehaviorDocument9 pagesConsumer Values, Product Benefits and Customer Value A Consumption Behaviorlyj1017No ratings yet
- Learning Theories/Models/Principles in Teaching ReadingDocument2 pagesLearning Theories/Models/Principles in Teaching Readingdarryl franciscoNo ratings yet
- 501 2019 0 B PDFDocument178 pages501 2019 0 B PDFMatomeNo ratings yet
- Test Bank For Social Psychology 5th Edition Tom GilovichDocument13 pagesTest Bank For Social Psychology 5th Edition Tom GilovichDevin MckayNo ratings yet
- Conference Paper Abstracts: International ManagementDocument91 pagesConference Paper Abstracts: International ManagementYet Barreda BasbasNo ratings yet
- Aubin. Seven-Step Palpation MethodDocument7 pagesAubin. Seven-Step Palpation MethodSofíaNo ratings yet
- LEARNING THEORIES Ausubel's Learning TheoryDocument17 pagesLEARNING THEORIES Ausubel's Learning TheoryCleoNo ratings yet
- Developmental TheoriesDocument12 pagesDevelopmental TheoriesLove clipseNo ratings yet
- Identity in Late AdulthoodDocument26 pagesIdentity in Late AdulthoodSamica_focaNo ratings yet
- Piaget-Assimilation Vs AccomodationDocument5 pagesPiaget-Assimilation Vs Accomodationboluwatife0000No ratings yet
- Final ResearchDocument42 pagesFinal ResearchGillian RamosNo ratings yet
- Eng02 Co1 ModuleDocument25 pagesEng02 Co1 ModuleRFSNo ratings yet
- Module 2 Lesson 2 - CADDocument8 pagesModule 2 Lesson 2 - CADMaryvic Bilan BusquitNo ratings yet
- Characters in Fictional Worlds - Understanding Imaginary Beings in Literature, Film, and Other Media (Revisionen Grundbegriffe Der Literaturtheorie 3)Document606 pagesCharacters in Fictional Worlds - Understanding Imaginary Beings in Literature, Film, and Other Media (Revisionen Grundbegriffe Der Literaturtheorie 3)masoha100% (5)
- Hypertext, Hypermedia and Multimedia: A ComparisonDocument25 pagesHypertext, Hypermedia and Multimedia: A ComparisonmimaNo ratings yet
- 005-CHAPTER IIDocument55 pages005-CHAPTER IIPISETH BONo ratings yet
- Theories of Development: Freud, Erikson, Piaget & KohlbergDocument39 pagesTheories of Development: Freud, Erikson, Piaget & KohlbergAlfonso Jr Quindoza100% (1)
- Content and Pedagogy in The Mother-Tongue Chapter 1Document25 pagesContent and Pedagogy in The Mother-Tongue Chapter 1Christy67% (6)
- Distored SchemasDocument14 pagesDistored SchemasJoelNo ratings yet
- research on gender stereotypes on highschool studentsDocument15 pagesresearch on gender stereotypes on highschool studentsrusselsanmillanNo ratings yet
- Extending Boundariesebook PDFDocument154 pagesExtending Boundariesebook PDFzZl3Ul2NNINGZzNo ratings yet
- GELECT2 ReviewerDocument30 pagesGELECT2 Reviewer20235701No ratings yet
- Why Good Thoughts Block Better Ones - The Mechanism of The Pernicious EinstellungDocument10 pagesWhy Good Thoughts Block Better Ones - The Mechanism of The Pernicious Einstellungxanod2003No ratings yet
- Cybernetics, Experience and The Concept of SelfDocument30 pagesCybernetics, Experience and The Concept of SelfLetricia VentinNo ratings yet
- HANA Tables ColumnStore Merges TokenOwners InternalDocument8 pagesHANA Tables ColumnStore Merges TokenOwners InternalHung PHAMNo ratings yet
- Jean Piaget's Cognitive TheoryDocument10 pagesJean Piaget's Cognitive TheoryBia KhanNo ratings yet