You might also like
- Arellano Charmaine Floor PlanDocument1 pageArellano Charmaine Floor PlanIvy Joama Barnachea PrioloNo ratings yet
- Prop En1065 C-D35Document1 pageProp En1065 C-D35alessandroNo ratings yet
- Lever Operated Dirctional Control Valve DL10Document4 pagesLever Operated Dirctional Control Valve DL10Riyaz SiddiqueNo ratings yet
- Eg135 S Airforce PDFDocument16 pagesEg135 S Airforce PDFMohammed AbdelsalamNo ratings yet
- Buck SimulariDocument12 pagesBuck SimulariBogdan Constantin 08No ratings yet
- Employability Skills 2nd Sem Final-148Document1 pageEmployability Skills 2nd Sem Final-148SAVITA MAURYANo ratings yet
- Girls HC Length To Weight 0.36moDocument1 pageGirls HC Length To Weight 0.36moHeart of the Valley, Pediatric CardiologyNo ratings yet
- Bar ChartDocument1 pageBar ChartMA. ZINA VIVIEN CABRERANo ratings yet
- Prop En1065 B-D30Document1 pageProp En1065 B-D30alessandroNo ratings yet
- 111 8014 0104 475 - R02 PDFDocument1 page111 8014 0104 475 - R02 PDFManish SharmaNo ratings yet
- Cotter Joint Drawing - Akash SavitaDocument1 pageCotter Joint Drawing - Akash SavitaEpicNewtonNo ratings yet
- Shema 1Document4 pagesShema 1Ali KENAANNo ratings yet
- GX 2 Psac 10 DRDocument20 pagesGX 2 Psac 10 DRfelipersbragaNo ratings yet
- XL120RTFCBDocument1 pageXL120RTFCBBigPantsNo ratings yet
- P01 Atterbrg PDFDocument1 pageP01 Atterbrg PDFDileep K NambiarNo ratings yet
- Atterberg Limits' Results: CL CHDocument1 pageAtterberg Limits' Results: CL CHDileep K NambiarNo ratings yet
- Valtra BH140Document10 pagesValtra BH140Puro Malte Bar & BurgerNo ratings yet
- Curso de Autocad 2023 Tc13: Revisions Rev. Description Rate Fernando RodríguezDocument1 pageCurso de Autocad 2023 Tc13: Revisions Rev. Description Rate Fernando RodríguezJosselyn BallesterosNo ratings yet
- Final 4 PDFDocument1 pageFinal 4 PDFBhuvanNo ratings yet
- GRCHRT Girls 24HdCirc-L4W 9210-NotagDocument1 pageGRCHRT Girls 24HdCirc-L4W 9210-NotagMohsin Saleem Mohsin saleemNo ratings yet
- CON - THIAM - MOUSTAPHA - Single Entry 30 Days - 2707235049Document1 pageCON - THIAM - MOUSTAPHA - Single Entry 30 Days - 2707235049ysow4140No ratings yet
- Section 6 Work EquipmentDocument40 pagesSection 6 Work EquipmentOscar Tello HuaripataNo ratings yet
- Alif Dan Rifki: Dept. Technical Reference Created by Approved byDocument1 pageAlif Dan Rifki: Dept. Technical Reference Created by Approved byAfifa AfifaNo ratings yet
- KS MFDocument2 pagesKS MFIhya UlumudinNo ratings yet
- AnshbisaryaDocument1 pageAnshbisaryaKrishna MoorthiNo ratings yet
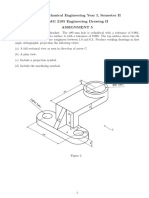
- EMG2105 Assignment5Document1 pageEMG2105 Assignment5Austin alasiriNo ratings yet
- Sample UkuranDocument2 pagesSample UkuranCici LiantiNo ratings yet
- Shape CodeDocument1 pageShape Codedejay100No ratings yet
- Plano BracketDocument1 pagePlano BracketAntonio Gonzalez VazquezNo ratings yet
- Colegio OkDocument1 pageColegio OkMaryorieDominguezNo ratings yet
- Electronics Dec Jan LRDocument149 pagesElectronics Dec Jan LRYakov NoginovNo ratings yet
- Ceiling Mounted Sirocco Ventilating Fans: FeaturesDocument1 pageCeiling Mounted Sirocco Ventilating Fans: FeaturesTYNo ratings yet
- Gear Pumps Motor gr.1 2 3 Catalogue ENGDocument184 pagesGear Pumps Motor gr.1 2 3 Catalogue ENGLuka JelovčanNo ratings yet
- Part2 - Sheet1Document1 pagePart2 - Sheet1Anwar HariryNo ratings yet
- Bodhran Folk FusionDocument1 pageBodhran Folk FusionAlberto Fernandez ValledorNo ratings yet
- HL757 7 (гидросхема)Document33 pagesHL757 7 (гидросхема)Nikolay KuznetsovNo ratings yet
- Wire Diagram - 1.默纳克 2019.01 FUJI 3000+ Electrical Schematic DiagramDocument26 pagesWire Diagram - 1.默纳克 2019.01 FUJI 3000+ Electrical Schematic DiagramTaeKook VKook100% (1)
- Ysrprofile PDFDocument5 pagesYsrprofile PDFSonia Esteves100% (1)
- View A: 1.1761.1134-2 Allowable Load Lashing Carrier G HMK 6 - 07Document1 pageView A: 1.1761.1134-2 Allowable Load Lashing Carrier G HMK 6 - 07altogarNo ratings yet
- EMX5000 PL (E) C PDFDocument61 pagesEMX5000 PL (E) C PDFJeff BrintonNo ratings yet
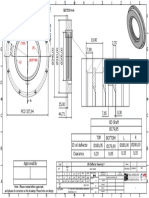
- Oil Deflector # 1 (ID SHAFT 179,85 MM)Document1 pageOil Deflector # 1 (ID SHAFT 179,85 MM)Danil AdityaNo ratings yet
- 3 3/4 Digit Multimeter: Users ManualDocument48 pages3 3/4 Digit Multimeter: Users ManualSANKARNo ratings yet
- Base P8 Plate 8Document1 pageBase P8 Plate 8AdeImanudinNo ratings yet
- Oil Deflector # 3 (ID SHAFT 530,00 MM)Document1 pageOil Deflector # 3 (ID SHAFT 530,00 MM)Danil AdityaNo ratings yet
- KS SPRDocument6 pagesKS SPRIhya UlumudinNo ratings yet
- Legrand 36252Document1 pageLegrand 36252helmi.rifkiNo ratings yet
- KS SPDocument4 pagesKS SPIhya UlumudinNo ratings yet
- Ujkcad3D1: Front View Scale: 1: 2 Milling N7 Milling N7Document1 pageUjkcad3D1: Front View Scale: 1: 2 Milling N7 Milling N7Rozy AlriadiNo ratings yet
- TFP Desen ExecutieDocument1 pageTFP Desen ExecutieCatalin9996No ratings yet
- Comem Oil Level Gauges With Magnetic JointDocument8 pagesComem Oil Level Gauges With Magnetic Jointcahya303No ratings yet
- 4 Section View A-A Scale: 1:1: Nita Ioan 14-May-20Document1 page4 Section View A-A Scale: 1:1: Nita Ioan 14-May-20Anonymous x10GM4rNo ratings yet
- Tack Weld PDFDocument1 pageTack Weld PDFAhmad LabiibNo ratings yet
- E:/hosuing - DWG, 27-07-2020 21:22:29, DWG To PDF - pc3Document1 pageE:/hosuing - DWG, 27-07-2020 21:22:29, DWG To PDF - pc3Sunil Kumar VemulaNo ratings yet
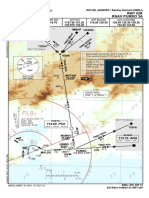
- SBRJ - Rnav Pumso 3a Rwy 02r - Sid - 20211007Document1 pageSBRJ - Rnav Pumso 3a Rwy 02r - Sid - 20211007FilipeDaumasNo ratings yet
- Curva S 1111Document1 pageCurva S 1111Jhon SuarezNo ratings yet
- TC13 RodríguezN PDFDocument1 pageTC13 RodríguezN PDFandres rodriguezNo ratings yet
- Receiver Philips AH709 Service ManualDocument8 pagesReceiver Philips AH709 Service ManualWilton CardosoNo ratings yet
- RoofingDocument24 pagesRoofinggenjing aracruNo ratings yet
- Database Management Systems: Understanding and Applying Database TechnologyFrom EverandDatabase Management Systems: Understanding and Applying Database TechnologyRating: 4 out of 5 stars4/5 (8)
- Soal Ujian Neuroscience 2012 HJD 1Document39 pagesSoal Ujian Neuroscience 2012 HJD 1Cox AbeeNo ratings yet
- Soal Ujian Neuroscience 2012 HJDDocument26 pagesSoal Ujian Neuroscience 2012 HJDCox AbeeNo ratings yet
- 8 Biliary System, PSPD, 2013Document21 pages8 Biliary System, PSPD, 2013Cox AbeeNo ratings yet
- 14 Asfek Operatif NyeriDocument55 pages14 Asfek Operatif NyeriCox AbeeNo ratings yet
- Kuliah Blok Neuroscience-SpineDocument27 pagesKuliah Blok Neuroscience-SpineCox AbeeNo ratings yet
- 2 Gastrointestinal System, FK, 2013Document73 pages2 Gastrointestinal System, FK, 2013Cox AbeeNo ratings yet
- Corrosive Lession of Esophagus: Wayan SuciptaDocument29 pagesCorrosive Lession of Esophagus: Wayan SuciptaCox AbeeNo ratings yet
- Digestion & Absorption: Dr. I Wayan Surudarma, M.SiDocument45 pagesDigestion & Absorption: Dr. I Wayan Surudarma, M.SiCox AbeeNo ratings yet
- Sampling MethodsDocument20 pagesSampling MethodsCox AbeeNo ratings yet
- Part 1Document6 pagesPart 1Cox AbeeNo ratings yet
- Dermatofitosis: Ema Surya Pertiwi (1102005108) Putu Mita Wulandari (1102005130)Document49 pagesDermatofitosis: Ema Surya Pertiwi (1102005108) Putu Mita Wulandari (1102005130)Cox AbeeNo ratings yet
- Higher Order Thinking Skills in The Classroom Skills: Bloom's TaxonomyDocument30 pagesHigher Order Thinking Skills in The Classroom Skills: Bloom's TaxonomyAhmad JawotoNo ratings yet
- Pedh Final g12 by Uncle Ervin and Others - Docx Version 1Document288 pagesPedh Final g12 by Uncle Ervin and Others - Docx Version 1Chu ChuNo ratings yet
- B Tech (CSE) FormatDocument5 pagesB Tech (CSE) FormatSwethank DasNo ratings yet
- James AtienzaDocument2 pagesJames Atienzaryan ravesNo ratings yet
- Reading JournalDocument2 pagesReading Journalapi-218358163No ratings yet
- 742 1 1 Final-Femaleconstable-SdDocument7 pages742 1 1 Final-Femaleconstable-SdDevender SoniNo ratings yet
- Basic Yoga Session - Yoga Exercise and Pose: The Sequence of Yoga AsanasDocument3 pagesBasic Yoga Session - Yoga Exercise and Pose: The Sequence of Yoga AsanasMurugan AnanthanNo ratings yet
- Genetics and Cytogenetics For UndergradsDocument145 pagesGenetics and Cytogenetics For UndergradsHarsh vardhanNo ratings yet
- Communication Studies IA - Kyle Rampaul (Final Draft)Document16 pagesCommunication Studies IA - Kyle Rampaul (Final Draft)Gamer XNo ratings yet
- Concept of Urban SociologyDocument4 pagesConcept of Urban SociologyDemmelash WannawNo ratings yet
- Detailed Lesson Plan in Arts Vi October 8Document3 pagesDetailed Lesson Plan in Arts Vi October 8Arlene DurbanNo ratings yet
- Last Flight of The Heyford K6875Document10 pagesLast Flight of The Heyford K6875James Watson100% (2)
- Aoife Kidney CV 2016 UpdatedDocument2 pagesAoife Kidney CV 2016 Updatedapi-352180955No ratings yet
- Chapter IV ResearchDocument18 pagesChapter IV ResearchNixon AtienzaNo ratings yet
- Collective Nouns Lesson PlanDocument3 pagesCollective Nouns Lesson PlanFlorr S90% (10)
- Chapter 1 - Entrepreneurship, Business and Entrepreneur Hien STDDocument109 pagesChapter 1 - Entrepreneurship, Business and Entrepreneur Hien STDHuy Hoàng PhanNo ratings yet
- DNA, Narco, BEAP Tests PDFDocument6 pagesDNA, Narco, BEAP Tests PDFSatyam Pathak100% (1)
- II.C.7 Temic Automotive v. Temic Automotive Phils. Employees Union, December 23, 2009Document4 pagesII.C.7 Temic Automotive v. Temic Automotive Phils. Employees Union, December 23, 2009Jin AghamNo ratings yet
- Activity SheetDocument2 pagesActivity Sheetapi-428047434No ratings yet
- Buddhist Pantheon - TendaiDocument3 pagesBuddhist Pantheon - TendaiMonge DorjNo ratings yet
- Breakeven in Units Contribuiton Margin RatioDocument11 pagesBreakeven in Units Contribuiton Margin RatioCookies And CreamNo ratings yet
- Indians Shed Their Inhibitions On HolidayDocument32 pagesIndians Shed Their Inhibitions On HolidayCharanjeev SalvaNo ratings yet
- Griffiths Consistent Quantum TheoryDocument407 pagesGriffiths Consistent Quantum TheoryVala Stola100% (5)
- Dcs - Chccsl001 - Task 1 Questions.v1.192401Document14 pagesDcs - Chccsl001 - Task 1 Questions.v1.192401spicy.issacNo ratings yet
- Drilling 1Document2 pagesDrilling 1luanlubisNo ratings yet
- Ca1 7Document104 pagesCa1 7Daryl GordoncilloNo ratings yet
- Chapter 11 Hormonal Coordination: 165 MinutesDocument60 pagesChapter 11 Hormonal Coordination: 165 MinutesAviBreezeNo ratings yet
- Power Quality Improvement at Nonlinear Loads UsingDocument14 pagesPower Quality Improvement at Nonlinear Loads UsingSuresh SrinivasanNo ratings yet
- The Jewish Targums and John's Logos TheologyDocument3 pagesThe Jewish Targums and John's Logos TheologyJim WestNo ratings yet
- A Survey of Network Traffic Monitoring and Analysis Tools PDFDocument24 pagesA Survey of Network Traffic Monitoring and Analysis Tools PDFDhitos MbombokNo ratings yet