You might also like
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 6 Urinary EliminationDocument5 pages6 Urinary EliminationkhautedameNo ratings yet
- Urinary CatheterizationDocument37 pagesUrinary CatheterizationCharles100% (2)
- Catheterization Procedure and Care GuidelinesDocument43 pagesCatheterization Procedure and Care GuidelinesJen Tirapan100% (2)
- Urinary Catheterization FemaleDocument13 pagesUrinary Catheterization Femaleroger100% (1)
- Catheterization and Perineal Care-PPT-1Document49 pagesCatheterization and Perineal Care-PPT-1AinaB Manalo100% (1)
- TracheostomyDocument35 pagesTracheostomyAbdur Raqib100% (1)
- How to Assist with Bedpans and UrinalsDocument8 pagesHow to Assist with Bedpans and UrinalsShereen AlobinayNo ratings yet
- Gloving and Degloving TechniqueDocument23 pagesGloving and Degloving TechniqueRichard PidlaoanNo ratings yet
- Checklist On Administering Cleansing Enema: ProcedureDocument3 pagesChecklist On Administering Cleansing Enema: ProcedureKyla CalzadoNo ratings yet
- Catheterization Procedure GuideDocument38 pagesCatheterization Procedure Guidedigantpathak100% (3)
- Colostomy Irrigation ProcedureDocument24 pagesColostomy Irrigation ProcedureJan Federick Bantay100% (1)
- Hot Sitz Bath Relieves PainDocument17 pagesHot Sitz Bath Relieves PainElaine Frances IlloNo ratings yet
- Urinary CatheterDocument4 pagesUrinary CatheterBindu SinghNo ratings yet
- Bed Bath & Bed ShampooDocument42 pagesBed Bath & Bed ShampooRusjen Claire Villamero100% (1)
- Catheterization DemoDocument48 pagesCatheterization Demojonna casumpangNo ratings yet
- 9 Intravenous TherapyDocument23 pages9 Intravenous TherapyKareem Mae Pines RaborNo ratings yet
- NCM - CatheterizationDocument3 pagesNCM - CatheterizationYanna Habib-MangotaraNo ratings yet
- Heart Assessment GuideDocument54 pagesHeart Assessment GuideMa. Carissa Allaine SantosNo ratings yet
- Nasogastric Tube Insertion: Nursing Guidelines and ConsiderationsDocument39 pagesNasogastric Tube Insertion: Nursing Guidelines and ConsiderationsTiger KneeNo ratings yet
- SuctioningDocument30 pagesSuctioningbajaoc60% (5)
- CVC Dressing Change ProcedureDocument1 pageCVC Dressing Change ProcedureAlexandra DtcNo ratings yet
- Bed BathDocument53 pagesBed BathAnnaAlfonso100% (1)
- Skin PreparationDocument3 pagesSkin Preparationmckulit_joey100% (2)
- TracheotomyDocument19 pagesTracheotomyKarina BundaNo ratings yet
- Surgical Gowning and GlovingDocument36 pagesSurgical Gowning and GlovingAudrie Allyson GabalesNo ratings yet
- St. Michael's College Nursing Suctioning GuideDocument7 pagesSt. Michael's College Nursing Suctioning Guideacademic purposesNo ratings yet
- Wound Care Procedure StudentsDocument2 pagesWound Care Procedure StudentsJan Philippe BelandoNo ratings yet
- 4 - Post Operative Nursing ManagementDocument38 pages4 - Post Operative Nursing ManagementraghadNo ratings yet
- Performing Urethral Urinary CatheterizationDocument4 pagesPerforming Urethral Urinary CatheterizationReyna Mee AhiyasNo ratings yet
- Calamba Doctors' College: Bachelor of Science in NursingDocument3 pagesCalamba Doctors' College: Bachelor of Science in NursingDaniel Daniel100% (1)
- Nursing Procedure Guide - Urinary Catheter InsertionDocument3 pagesNursing Procedure Guide - Urinary Catheter Insertionmharmukim03No ratings yet
- Urinary CatheterizationDocument3 pagesUrinary CatheterizationbabyrainbowNo ratings yet
- Nasogastric Tube InsertionDocument3 pagesNasogastric Tube Insertionmarie100% (5)
- Medication AdministrationDocument298 pagesMedication AdministrationOfficially RandomNo ratings yet
- Vital SignsDocument13 pagesVital SignsMarcus, RN100% (3)
- Proper Perineal Care TechniquesDocument3 pagesProper Perineal Care TechniquesParado Cabañal SkylieghNo ratings yet
- SuctioningDocument31 pagesSuctioningmelanie silvaNo ratings yet
- StomaDocument37 pagesStomaAndryHarisNo ratings yet
- Lab 2 Nursing Skill - Vital Sings 2021Document10 pagesLab 2 Nursing Skill - Vital Sings 2021PHOEBE Ci100% (1)
- Performance Checklist - Perineal CareDocument2 pagesPerformance Checklist - Perineal Careshubham vermaNo ratings yet
- Scrubbing Gowning and Gloving LECTUREDocument5 pagesScrubbing Gowning and Gloving LECTUREEyji GeronimoNo ratings yet
- Colostomy IrrigationDocument2 pagesColostomy IrrigationAudreySalvadorNo ratings yet
- Colostomy CareDocument49 pagesColostomy Caregladz25100% (1)
- A. Bedbath: Definition: PurposesDocument2 pagesA. Bedbath: Definition: PurposesKyla100% (1)
- Perinal Care FemaleDocument1 pagePerinal Care FemaleRaquel M. MendozaNo ratings yet
- M Digestion" Absorption" EliminationDocument104 pagesM Digestion" Absorption" EliminationChristine Carol FilipinasNo ratings yet
- Surgical HandwashingDocument1 pageSurgical HandwashingWeng RamojalNo ratings yet
- IV TherapyDocument39 pagesIV TherapyChannelGNo ratings yet
- NCM 109 Skills ChecklistDocument8 pagesNCM 109 Skills ChecklistReygine CariñoNo ratings yet
- Assessing Learners' Characteristics, Needs and StylesDocument56 pagesAssessing Learners' Characteristics, Needs and StylesBryan Nartatez Bautista100% (1)
- 8.Gastro-Intestinal System DisordersDocument251 pages8.Gastro-Intestinal System Disordersgold man100% (1)
- Standard Precautions: (If You Have Questions, Go To Nurse Station)Document8 pagesStandard Precautions: (If You Have Questions, Go To Nurse Station)Farah Fauziah Rachmawatie100% (1)
- Urethral Catheterization 1Document31 pagesUrethral Catheterization 1Hilman HadiansyahNo ratings yet
- Perineal Genital Care PERFORMANCE-CHECKLISTDocument2 pagesPerineal Genital Care PERFORMANCE-CHECKLISTMary joy PaaNo ratings yet
- Fundamentals of Nursing: OxygenationDocument56 pagesFundamentals of Nursing: OxygenationFEVIE ANNE BANATAONo ratings yet
- Bed Bath ProcedureDocument4 pagesBed Bath ProcedureMarku LeeNo ratings yet
- Colostomy Ileostomy CareDocument6 pagesColostomy Ileostomy Careأبوأحمد الحكيمNo ratings yet
- Iv CannulationDocument6 pagesIv Cannulation2013SecBNo ratings yet
- CatheterizationDocument23 pagesCatheterizationyuuki konnoNo ratings yet
- 2.4 165880-2011-League - of - Cities - of - The - Phils. - v. - Commission20180914-5466-UtnhegDocument27 pages2.4 165880-2011-League - of - Cities - of - The - Phils. - v. - Commission20180914-5466-UtnhegBiancaDiwaraNo ratings yet
- Congruent FiguresDocument18 pagesCongruent FiguresMaria MargaritaNo ratings yet
- G.R. No. L-27811 Lacson-Magallanes Co v. Jose PañoDocument1 pageG.R. No. L-27811 Lacson-Magallanes Co v. Jose PañoZen Joaquin100% (1)
- Heart Failure Drugs-Critical Thinking Short Case StudiesDocument1 pageHeart Failure Drugs-Critical Thinking Short Case StudiesMaria MargaritaNo ratings yet
- Math ReviewDocument14 pagesMath ReviewMaria MargaritaNo ratings yet
- Vascular Access and Infusion TherapyDocument47 pagesVascular Access and Infusion TherapyMaria Margarita100% (1)
- League of Cities of the Philippines v. Commission on ElectionsDocument15 pagesLeague of Cities of the Philippines v. Commission on ElectionsJia Chu ChuaNo ratings yet
- Nursing From Conception To AdolescenceDocument24 pagesNursing From Conception To AdolescenceMaria MargaritaNo ratings yet
- 16 A 4 BsubjectsDocument70 pages16 A 4 BsubjectsDanish AlamNo ratings yet
- RS 14 95 de Me NT IaDocument80 pagesRS 14 95 de Me NT IaMaria MargaritaNo ratings yet
- Rita SantiagoDocument3 pagesRita SantiagoMaria MargaritaNo ratings yet
- 2 Perinatal Care To PostDocument49 pages2 Perinatal Care To PostMaria MargaritaNo ratings yet
- Ateneo 2007 Political Law (Public International Law)Document12 pagesAteneo 2007 Political Law (Public International Law)Al SimbajonNo ratings yet
- Inflammation and Healing (Revised/Reviewed)Document35 pagesInflammation and Healing (Revised/Reviewed)Maria MargaritaNo ratings yet
- Gold Standard For NclexDocument113 pagesGold Standard For NclexMaria Margarita86% (29)
- Route/Dosage: Concentration: Not To Exceed 10 Mg/ml. Do NotDocument2 pagesRoute/Dosage: Concentration: Not To Exceed 10 Mg/ml. Do NotMaria MargaritaNo ratings yet
- Cancer and EOLDocument114 pagesCancer and EOLMaria MargaritaNo ratings yet
- Anxiety, Obsessive-Compulsive, and Related DisordersDocument20 pagesAnxiety, Obsessive-Compulsive, and Related DisordersMaria MargaritaNo ratings yet
- CLIN 1330 Week 7 Complex Wound Care Spring 2018Document26 pagesCLIN 1330 Week 7 Complex Wound Care Spring 2018Maria MargaritaNo ratings yet
- 2016 NUR1021 Calculation of Basic IV Drip Rates - InstructorDocument39 pages2016 NUR1021 Calculation of Basic IV Drip Rates - InstructorMikhaelEarlSantosTacorda100% (1)
- Respiratory SystemDocument90 pagesRespiratory SystemMaria MargaritaNo ratings yet
- CPALE Syllabi 2018 PDFDocument32 pagesCPALE Syllabi 2018 PDFLorraine TomasNo ratings yet
- Antibiotics Part 2 - Student-Self Study PowerPoint Presentation NotesDocument27 pagesAntibiotics Part 2 - Student-Self Study PowerPoint Presentation NotesMaria MargaritaNo ratings yet
- Conflicts Case Digest CompilationDocument10 pagesConflicts Case Digest CompilationSuzieNo ratings yet
- Antibiotics Part 1 - Student-Self Study PowerPoint Presentation NotesDocument63 pagesAntibiotics Part 1 - Student-Self Study PowerPoint Presentation NotesMaria MargaritaNo ratings yet
- Bipolar DisorderDocument20 pagesBipolar DisorderMaria MargaritaNo ratings yet
- Conflicts Case Digest CompilationDocument10 pagesConflicts Case Digest CompilationSuzieNo ratings yet
- 2 Perinatal Care To PostDocument49 pages2 Perinatal Care To PostMaria MargaritaNo ratings yet
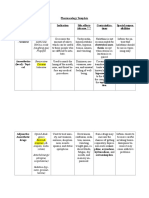
- Pharmacology Template Classification Examples Indication Side Effects Adverse Contraindica-Tions Special Respon - SibilitiesDocument3 pagesPharmacology Template Classification Examples Indication Side Effects Adverse Contraindica-Tions Special Respon - SibilitiesMaria MargaritaNo ratings yet
- Emergency Preparedness Plan EssentialsDocument78 pagesEmergency Preparedness Plan EssentialsHuey Calabines50% (2)
- Kualitas Tidur dan Kecemasan pada MahasiswaDocument7 pagesKualitas Tidur dan Kecemasan pada MahasiswaRamayanaNo ratings yet
- GCF Annual Report 2022-78p PDFDocument78 pagesGCF Annual Report 2022-78p PDFbaccalaNo ratings yet
- عشر امتحانات للصف الثالث الثانوي - هدية من ماي نيو فريندDocument66 pagesعشر امتحانات للصف الثالث الثانوي - هدية من ماي نيو فريندsayed SalehNo ratings yet
- Doloplus 2 ToolDocument3 pagesDoloplus 2 ToolHaMy NguyenNo ratings yet
- C0003 NHLDocument450 pagesC0003 NHLVasudev BhanajiNo ratings yet
- Third World Aid EssayDocument3 pagesThird World Aid EssayEstefania UribeNo ratings yet
- Explanation of BenefitsDocument1 pageExplanation of Benefitsmohamed hamedNo ratings yet
- MJP Tips and InfoDocument4 pagesMJP Tips and InfonatyaNo ratings yet
- In Memoriam: Renowned Psychiatrist and Author Sir David Hawkins 1927-2012Document2 pagesIn Memoriam: Renowned Psychiatrist and Author Sir David Hawkins 1927-2012Aditya VarunNo ratings yet
- Urine Indican Excretion in Malabsorptive DisordersDocument8 pagesUrine Indican Excretion in Malabsorptive DisordersBiancake Sta. AnaNo ratings yet
- People's Vision for Mumbai's DevelopmentDocument86 pagesPeople's Vision for Mumbai's DevelopmentAravind UnniNo ratings yet
- Nursing Care Plan - Acute Pain Related To Surgical IncisionDocument2 pagesNursing Care Plan - Acute Pain Related To Surgical IncisionCamilogs80% (10)
- Cerebral Palsy Care Giving GuideDocument511 pagesCerebral Palsy Care Giving GuideJoel OntiverosNo ratings yet
- Republic of The Philippines 9173Document2 pagesRepublic of The Philippines 9173jansestacioNo ratings yet
- Moribund ICDSDocument114 pagesMoribund ICDSVikas SamvadNo ratings yet
- Dela Torre vs Imbuido and Cruz vs Agas medical malpractice casesDocument19 pagesDela Torre vs Imbuido and Cruz vs Agas medical malpractice casesLenette LupacNo ratings yet
- The Features and Benefits of Broiler Starter Feeds That Include Alphasoy™Document31 pagesThe Features and Benefits of Broiler Starter Feeds That Include Alphasoy™Matute SalmonNo ratings yet
- AFIU Post Op Managment of Renal Transplant - Prof Saeed AkhtarDocument55 pagesAFIU Post Op Managment of Renal Transplant - Prof Saeed AkhtarUmar FarooqNo ratings yet
- Acp CBC 1Document52 pagesAcp CBC 1Danny R. SalvadorNo ratings yet
- PE UNIT 1 Active Recreation (Lifestyle and Weight Management)Document26 pagesPE UNIT 1 Active Recreation (Lifestyle and Weight Management)Charmaine RamosNo ratings yet
- Psychology Learning Objectives, Contents, Activities and EvaluationDocument12 pagesPsychology Learning Objectives, Contents, Activities and EvaluationSAYMABANUNo ratings yet
- Ahf Academy Lambrinou Case 1 17september2015.ppsxDocument36 pagesAhf Academy Lambrinou Case 1 17september2015.ppsxMWNo ratings yet
- 6 Best Homeopathic Medicines For Swollen Ankles - Homeopathy at DrHomeoDocument9 pages6 Best Homeopathic Medicines For Swollen Ankles - Homeopathy at DrHomeovivek khannaNo ratings yet
- Gastroenteritis Case ReportDocument12 pagesGastroenteritis Case ReportjisooNo ratings yet
- Organisational Change and Stress ManagementDocument18 pagesOrganisational Change and Stress ManagementDisha GanatraNo ratings yet
- IMAEC Disinfectant Product Catalogue - DigitalCopy - April - 2023Document32 pagesIMAEC Disinfectant Product Catalogue - DigitalCopy - April - 2023ToureNo ratings yet
- Jamaica Society For The Blind (JSB)Document4 pagesJamaica Society For The Blind (JSB)eyecarecaribbeanNo ratings yet
- Psychiatric History and Mental Status Exam TechniquesDocument16 pagesPsychiatric History and Mental Status Exam TechniquesMangayarkarasi ChandrakasanNo ratings yet
- GMP and Preparation in Hospital Pharmacies - Bouwman and Andersen 19 (5) - 469 - European Journal of Hospital Pharmacy - Science and PracticeDocument4 pagesGMP and Preparation in Hospital Pharmacies - Bouwman and Andersen 19 (5) - 469 - European Journal of Hospital Pharmacy - Science and Practicecarbou0% (1)