You might also like
- National Health Strategy For Zimbabwe (2021 - 2025)Document104 pagesNational Health Strategy For Zimbabwe (2021 - 2025)Praise Nehumambi100% (6)
- Prophecy Neuro ICU Exam Content OutlineDocument5 pagesProphecy Neuro ICU Exam Content OutlineDarren DawkinsNo ratings yet
- Criteria For The Ideal Treatment Option For Failed Tics Surgical or NonsurgicalDocument8 pagesCriteria For The Ideal Treatment Option For Failed Tics Surgical or NonsurgicalPaRpArOsSaNo ratings yet
- Endodontics Final ReviewerDocument27 pagesEndodontics Final ReviewerRosette Go100% (5)
- Endodontics Final ReviewerDocument16 pagesEndodontics Final ReviewerMehdi Moshaveri100% (3)
- Serial ExtractionDocument38 pagesSerial ExtractionRamy HanyNo ratings yet
- Endomishaps SeminarDocument44 pagesEndomishaps SeminarSuma TettaNo ratings yet
- Endodontic Mishaps: IDocument9 pagesEndodontic Mishaps: IMariyam AnzilNo ratings yet
- Microsoft Word - Endodontic - MishapsDocument20 pagesMicrosoft Word - Endodontic - MishapsShufeiNo ratings yet
- Asalaam Alekkum: DR Gaurav Garg, Lecturer College of Dentistry, Al Zulfi, MUDocument57 pagesAsalaam Alekkum: DR Gaurav Garg, Lecturer College of Dentistry, Al Zulfi, MUMaGe IsTeNo ratings yet
- 13 6 Endodontic Mishaps PDFDocument20 pages13 6 Endodontic Mishaps PDFzaheerbdsNo ratings yet
- Endodontic Mishaps 1Document10 pagesEndodontic Mishaps 1علي صادق جعفرNo ratings yet
- Causes of Endodontic FailuresDocument8 pagesCauses of Endodontic Failuresizeldien5870No ratings yet
- Endodontic RetreatmentDocument59 pagesEndodontic RetreatmentOmar MustafaNo ratings yet
- Endodontic SurgeryDocument8 pagesEndodontic SurgeryjoseNo ratings yet
- Goldfein JOE 2013Document4 pagesGoldfein JOE 2013NonoNo ratings yet
- Endodontic MishapsDocument199 pagesEndodontic Mishapsrasagna reddy100% (4)
- Articulo de Endodoncia PDFDocument14 pagesArticulo de Endodoncia PDFJuan Pablo Rondon OyuelaNo ratings yet
- Practice: Tooth Preparation For Post-Retained RestorationsDocument9 pagesPractice: Tooth Preparation For Post-Retained RestorationsSitiKhadijahNo ratings yet
- 5 - Procedural AccidentsDocument12 pages5 - Procedural AccidentsPrince AhmedNo ratings yet
- 11.endodontic MishapsDocument27 pages11.endodontic MishapsRiya JainNo ratings yet
- Basics of Root Canal TreatmentDocument117 pagesBasics of Root Canal TreatmentSameer VinchurkarNo ratings yet
- Bleaching3 Konser2Document3 pagesBleaching3 Konser2akmalsatibiNo ratings yet
- Instrument RetrievalDocument37 pagesInstrument RetrievalPraveen JohnNo ratings yet
- Endodontic MishapsDocument41 pagesEndodontic MishapsDrKaran Khaneja100% (4)
- Brighter Futures - Orthodontic Endodontic Considerations Part 2Document4 pagesBrighter Futures - Orthodontic Endodontic Considerations Part 2Valonia IreneNo ratings yet
- Pulpal Therapy in PrimaryDocument34 pagesPulpal Therapy in PrimaryShahid HameedNo ratings yet
- Repair of Teeth With Cracks in CrownsDocument52 pagesRepair of Teeth With Cracks in CrownsSandeep PksNo ratings yet
- 10 4 2013Document49 pages10 4 2013Anonymous 2h5lIeNo ratings yet
- Endodontic RetreatmentDocument14 pagesEndodontic Retreatmentrojek63No ratings yet
- Management of An Endodontic-Periodontal Lesion Caused by IatrogenicDocument8 pagesManagement of An Endodontic-Periodontal Lesion Caused by IatrogenicDebora GultomNo ratings yet
- Endodontics Procedural ErrorsDocument4 pagesEndodontics Procedural ErrorsHimasai Reddy VangaNo ratings yet
- Scope of Endodontics: DefinitionDocument5 pagesScope of Endodontics: DefinitionRana SayedNo ratings yet
- Retrospective Study On Efficacy of Intermaxillary Fixation ScrewsDocument3 pagesRetrospective Study On Efficacy of Intermaxillary Fixation ScrewsPorcupine TreeNo ratings yet
- Treatment of Acute and Chronic PeriodontitisDocument66 pagesTreatment of Acute and Chronic PeriodontitisBikku NegiNo ratings yet
- Endodontic Managementof Fourrootedpremolar JCD2013Document4 pagesEndodontic Managementof Fourrootedpremolar JCD2013Lucas PeixotoNo ratings yet
- Neelesh K BanjareDocument37 pagesNeelesh K BanjareShrikant HoskereNo ratings yet
- Treatment For ChildrenDocument66 pagesTreatment For ChildrenMohsin HabibNo ratings yet
- Dr. Muneera GhaithanDocument44 pagesDr. Muneera GhaithanAli MezaalNo ratings yet
- Endodontic Update 2006Document21 pagesEndodontic Update 2006James LinNo ratings yet
- Four Impacted Fourth Molars in A Young Patient: A Case ReportDocument5 pagesFour Impacted Fourth Molars in A Young Patient: A Case ReportPo PowNo ratings yet
- Rationale For RetreatmentDocument8 pagesRationale For RetreatmentAbhiram BalanNo ratings yet
- 113 Canal EnlargmentDocument10 pages113 Canal Enlargmentpoulak08No ratings yet
- Mouth Preparation: DR - Mona Galal Lecturer at Prosthodontics DepartmentDocument70 pagesMouth Preparation: DR - Mona Galal Lecturer at Prosthodontics DepartmentAbdelrhman AdelNo ratings yet
- Lec. Deep CariesDocument47 pagesLec. Deep CariesMaria EvergardenNo ratings yet
- Surgical EndoDocument16 pagesSurgical EndoTraian IlieNo ratings yet
- Effectiveness of XP Endo Finisher & XP-Endo Finisher RDocument63 pagesEffectiveness of XP Endo Finisher & XP-Endo Finisher Rrasagna reddyNo ratings yet
- Endodontic Management of Taurodontism in Maxillary Molar: A Case ReportDocument4 pagesEndodontic Management of Taurodontism in Maxillary Molar: A Case ReportMeidi KurniaNo ratings yet
- Endodontic Treatment FailureDocument8 pagesEndodontic Treatment FailureHawzheen SaeedNo ratings yet
- Endodontic AccessDocument5 pagesEndodontic AccessShyambhavi SrivastavaNo ratings yet
- Retreatment in Persistent Apical PeriodontitisDocument169 pagesRetreatment in Persistent Apical PeriodontitisAnciya NazarNo ratings yet
- Accidents in Endodontic A Case ReportDocument4 pagesAccidents in Endodontic A Case ReportDr.O.R.GANESAMURTHINo ratings yet
- Factors That Cause Endodontic Failures in GeneralDocument5 pagesFactors That Cause Endodontic Failures in GeneralSdffNo ratings yet
- Endodontic Retreatment in Case of Failure: Case ReportDocument3 pagesEndodontic Retreatment in Case of Failure: Case ReportputriraudatulNo ratings yet
- Clinical Management of Endodontic CasesDocument91 pagesClinical Management of Endodontic CasesSharlene OngNo ratings yet
- Endodontic MishapsDocument19 pagesEndodontic MishapsSayak GuptaNo ratings yet
- Ipc DPCDocument72 pagesIpc DPCSarath MohanNo ratings yet
- Endo Instruments and MaterialsDocument131 pagesEndo Instruments and MaterialsIndrani DasNo ratings yet
- 16 Access Related Endodontic Mishaps.20170115064301Document8 pages16 Access Related Endodontic Mishaps.20170115064301Amrutha DasariNo ratings yet
- Minimally Invasive Approaches in Endodontic PracticeFrom EverandMinimally Invasive Approaches in Endodontic PracticeGianluca PlotinoNo ratings yet
- Esthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsFrom EverandEsthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsRichard D. TrushkowskyNo ratings yet
- Normal Aging: Vaishali Singhal DMD, PHD, MsDocument68 pagesNormal Aging: Vaishali Singhal DMD, PHD, MsroorayNo ratings yet
- 12-Metal-Ceramic RestorationsDocument30 pages12-Metal-Ceramic RestorationsroorayNo ratings yet
- Health Advice: Sorting It Out For Patients and For YourselfDocument37 pagesHealth Advice: Sorting It Out For Patients and For YourselfroorayNo ratings yet
- Principles in Dental Public Health: © AaphdDocument87 pagesPrinciples in Dental Public Health: © AaphdroorayNo ratings yet
- O-Chem Day 1-Basics NomenclatureDocument2 pagesO-Chem Day 1-Basics NomenclatureroorayNo ratings yet
- Solutions Test 3Document4 pagesSolutions Test 3roorayNo ratings yet
- Menstrual HygieneDocument6 pagesMenstrual HygieneKalyan PaulNo ratings yet
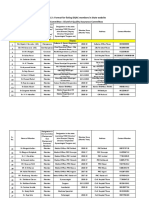
- ANNEX DQAC Member List 29 OctDocument29 pagesANNEX DQAC Member List 29 OctSpace HR100% (2)
- PeritonitisDocument21 pagesPeritonitischrisyenNo ratings yet
- The Clinical Role of Community PharmacistDocument89 pagesThe Clinical Role of Community PharmacistBIANCA KARLA LICATANNo ratings yet
- Ich GCP: HistoryDocument57 pagesIch GCP: HistoryChandrashekhar Singh100% (1)
- NCP Acute PainDocument7 pagesNCP Acute PainIvan PulancoNo ratings yet
- Ectopic PregnancyDocument7 pagesEctopic PregnancyﺳﻮﺘﻴﺎﺳﻴﻪNo ratings yet
- UNEP Directory March 2021Document34 pagesUNEP Directory March 2021Perera KusalNo ratings yet
- Yayie Case PresentationDocument12 pagesYayie Case PresentationYayie Querubin SilvestreNo ratings yet
- Department of Health & Human ServicesDocument11 pagesDepartment of Health & Human ServicesJoelNo ratings yet
- The Unified E-Medical Record v2.1Document18 pagesThe Unified E-Medical Record v2.1Alexandra BotezatuNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument38 pagesEVMS Critical Care COVID-19 ProtocolDrivailaNo ratings yet
- Epigenetics Congress 2018 BookDocument120 pagesEpigenetics Congress 2018 BookAnonymous FoOawtbV8No ratings yet
- Practical Year Logbook For Students in The Term: OphthalmologyDocument20 pagesPractical Year Logbook For Students in The Term: OphthalmologyDimpi DeviNo ratings yet
- Shehryar Baig Resume 2Document2 pagesShehryar Baig Resume 2api-491306844No ratings yet
- PRC-BON Memorandum Order No. 1-b Series of 2009Document2 pagesPRC-BON Memorandum Order No. 1-b Series of 2009PhilippineNursingDirectory.comNo ratings yet
- Case Presentation On Normal Pregnancy: Moderator: DR Saravana Prakash Presentor: DR PremDocument12 pagesCase Presentation On Normal Pregnancy: Moderator: DR Saravana Prakash Presentor: DR PremPrem JepinaNo ratings yet
- Singrauli - PIP ReportDocument29 pagesSingrauli - PIP Reportgaurav chauhanNo ratings yet
- ADALIMUMAB (Humira)Document4 pagesADALIMUMAB (Humira)GLen CaniedoNo ratings yet
- A Study On Knowledge On Selected Minor Disorders of Newborn Among Postnatal Mothers in A Selected Hospital at MangaluruDocument7 pagesA Study On Knowledge On Selected Minor Disorders of Newborn Among Postnatal Mothers in A Selected Hospital at Mangaluruسمية الورادNo ratings yet
- Implementation of An Oxytocin Checklist To Improve.3Document6 pagesImplementation of An Oxytocin Checklist To Improve.3Em Wahyu ArNo ratings yet
- Turquoise Lodge Brochure 2020Document2 pagesTurquoise Lodge Brochure 2020Ryan MalsNo ratings yet
- English For Pharmacy Students - 21. - 22.12Document1 pageEnglish For Pharmacy Students - 21. - 22.12George UrtilaNo ratings yet
- Exploring School Nurse Interventions and Health and Education Outcomes: An Integrative ReviewDocument14 pagesExploring School Nurse Interventions and Health and Education Outcomes: An Integrative ReviewpaoNo ratings yet
- Psychiatric Nursing Set 1 Oct 27Document8 pagesPsychiatric Nursing Set 1 Oct 27Jayrald CruzadaNo ratings yet
- Trifold BrochureDocument2 pagesTrifold BrochureRendanLumbertNo ratings yet
- Community-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaDocument15 pagesCommunity-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaMajo EscobarNo ratings yet
- Deemed Stray Vacancy Round Seats PG MD - Ms - DiplomaDocument39 pagesDeemed Stray Vacancy Round Seats PG MD - Ms - DiplomaManoj KashyapNo ratings yet