You might also like
- Radiologic Technology: As A ProfessionDocument30 pagesRadiologic Technology: As A ProfessionKim MngcupaNo ratings yet
- Understanding Chronic Kidney Disease: A guide for the non-specialistFrom EverandUnderstanding Chronic Kidney Disease: A guide for the non-specialistRating: 4 out of 5 stars4/5 (3)
- Ruiz Renal 2017Document70 pagesRuiz Renal 2017Em AsumbradoNo ratings yet
- Unit 2 - Design Principles and MethodsDocument45 pagesUnit 2 - Design Principles and Methodsmaya_muthNo ratings yet
- How To Position Finerenone in The Treatment Algorithm For Type 2 Diabetes With Renal Complication - GPMPDocument27 pagesHow To Position Finerenone in The Treatment Algorithm For Type 2 Diabetes With Renal Complication - GPMPTaufiqurrokhman RofiiNo ratings yet
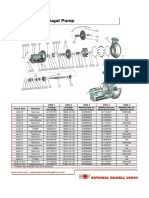
- Mission Magnum I Pump Spare PartsDocument2 pagesMission Magnum I Pump Spare PartsEleazar GallegosNo ratings yet
- Reverse LogisticsDocument21 pagesReverse LogisticsParth V. PurohitNo ratings yet
- 1) Cir v. Marubeni Corp-Duya (d2017)Document1 page1) Cir v. Marubeni Corp-Duya (d2017)joyceNo ratings yet
- H940C PartsDocument388 pagesH940C PartsRildo ChavesNo ratings yet
- DR Arwedi Inisiasi HD Pit 2018Document28 pagesDR Arwedi Inisiasi HD Pit 2018Aulia Achmad Yudha PratamaNo ratings yet
- Chronic Kidney Disease: The BasicsDocument56 pagesChronic Kidney Disease: The BasicsAlmas Safina KauserNo ratings yet
- ME 205 ThermodynamicsDocument3 pagesME 205 Thermodynamicsnandan144No ratings yet
- Medication Safety inCKDDocument56 pagesMedication Safety inCKDFransisca Dhani KurniasihNo ratings yet
- Boala Cronica de Rinichi Adrian CovicDocument85 pagesBoala Cronica de Rinichi Adrian CovicLorenaNo ratings yet
- Approach To GI BleedDocument97 pagesApproach To GI BleedPankaj IngleNo ratings yet
- Dr. Hani - Cardiorenal Syndrome 2020Document33 pagesDr. Hani - Cardiorenal Syndrome 2020lab adjidarmoNo ratings yet
- DR Aida Lombok 3 Mei 2017 - HisfarsiDocument39 pagesDR Aida Lombok 3 Mei 2017 - HisfarsiBasri BaslamNo ratings yet
- Chronic Kidney Disease Bhakti MuliaDocument24 pagesChronic Kidney Disease Bhakti MuliaCOVID RSHJNo ratings yet
- AKI Vs CKD Lecture Latest 3rd Dec 2018Document51 pagesAKI Vs CKD Lecture Latest 3rd Dec 2018mugilessNo ratings yet
- 02-50-4079 ABB ManagingTransRecipBk PC PDFDocument12 pages02-50-4079 ABB ManagingTransRecipBk PC PDFjulma1306No ratings yet
- IraposopemidososDocument9 pagesIraposopemidososjoseNo ratings yet
- 1986 AKI Primary PreventionDocument30 pages1986 AKI Primary PreventionSid DhayriNo ratings yet
- Anemia: Chronic Kidney DiseaseDocument12 pagesAnemia: Chronic Kidney DiseasetyasNo ratings yet
- Post Cardiac Surgery AkiDocument72 pagesPost Cardiac Surgery AkiMehdi BakhshiNo ratings yet
- The Challenge of Kidney Damage During Interventional Cardiology ProceduresDocument6 pagesThe Challenge of Kidney Damage During Interventional Cardiology ProceduresIJAR JOURNALNo ratings yet
- Actualizaciones Sobre La Enfermedad Renal PoliquísticaDocument45 pagesActualizaciones Sobre La Enfermedad Renal PoliquísticaEvelyn CaveroNo ratings yet
- Presentation of CKDDocument40 pagesPresentation of CKDandi hikmasharyNo ratings yet
- Circoutcomes 117 003665Document6 pagesCircoutcomes 117 003665M EhabNo ratings yet
- 1 Sepsis 1Document109 pages1 Sepsis 1aliNo ratings yet
- Best Practices in Renal Dosing: Bruce A. Mueller, PharmdDocument47 pagesBest Practices in Renal Dosing: Bruce A. Mueller, PharmdRuqayya AdamuNo ratings yet
- Nephropathy With Intravenous ContrastDocument9 pagesNephropathy With Intravenous Contrastjose torresNo ratings yet
- Living Donor Kidney Transplantation - Jonathon Oldsburgh - UOM 21.8.19Document106 pagesLiving Donor Kidney Transplantation - Jonathon Oldsburgh - UOM 21.8.19Renal Association MauritiusNo ratings yet
- IsekiDocument6 pagesIsekiM. Putra Ardhimas KesumaNo ratings yet
- Acute Kidney Injury: Mohammad RudiansyahDocument80 pagesAcute Kidney Injury: Mohammad Rudiansyahshrt gtNo ratings yet
- Aki Vs CKD: Consultant NephrologistDocument35 pagesAki Vs CKD: Consultant NephrologistFreeburn SimunchembuNo ratings yet
- Preventif CKD FinalDocument43 pagesPreventif CKD Finaltika.dyahmustikaNo ratings yet
- Pharmacotherapy in Chronic Kidney Disease Patients Presenting With Acute Coronary SyndromeDocument27 pagesPharmacotherapy in Chronic Kidney Disease Patients Presenting With Acute Coronary SyndromeaudiNo ratings yet
- Molen2018 Article Post-contrastAcuteKidneyInjury PDFDocument11 pagesMolen2018 Article Post-contrastAcuteKidneyInjury PDFEliza CrăciunNo ratings yet
- Primary Care - Nephrology Interface: Providing Coordinated CKD CareDocument158 pagesPrimary Care - Nephrology Interface: Providing Coordinated CKD CarecamidocNo ratings yet
- Approach To Acute Kidney InjuryDocument44 pagesApproach To Acute Kidney InjuryKue GosongNo ratings yet
- 2008bns 0829 0900 02Document71 pages2008bns 0829 0900 02Asep ArdiNo ratings yet
- StemiDocument29 pagesSteminadia shabriNo ratings yet
- DR Vito Vascular ApicdDocument32 pagesDR Vito Vascular ApicdluckyariadneeNo ratings yet
- Kidney Disease in Patients With HIV Infection and AIDS: InvitedarticleDocument9 pagesKidney Disease in Patients With HIV Infection and AIDS: InvitedarticleAryanto DedyNo ratings yet
- CKD Talk To Medical Update GroupDocument49 pagesCKD Talk To Medical Update GroupRenal Association MauritiusNo ratings yet
- Linician Pdate: Contrast-Induced NephropathyDocument6 pagesLinician Pdate: Contrast-Induced NephropathyayupurnamasariiNo ratings yet
- Chapter 102 Medical Management of The Kidney Transplant Recipient Cardiovascular Disease and Other IssuesDocument11 pagesChapter 102 Medical Management of The Kidney Transplant Recipient Cardiovascular Disease and Other Issuesadrian mendoza croesNo ratings yet
- CHRONIC KIDNEY DISEASE Pelatihan Perawat HD 2021Document33 pagesCHRONIC KIDNEY DISEASE Pelatihan Perawat HD 2021Yudha WirawanNo ratings yet
- Atrial Fibrillation and Thromboembolism in Patients With Chronic Kidney DiseaseDocument13 pagesAtrial Fibrillation and Thromboembolism in Patients With Chronic Kidney Diseasetenty isniNo ratings yet
- Acute Renal Failure: From Basics To The Latest AdvancesDocument120 pagesAcute Renal Failure: From Basics To The Latest AdvancesAfifa Prima GittaNo ratings yet
- PCP in A Box - Module 1Document43 pagesPCP in A Box - Module 1Fate ChanNo ratings yet
- Cardiovascular Complication in HD 2019 DR RubinDocument49 pagesCardiovascular Complication in HD 2019 DR RubinASIS ADRINo ratings yet
- Cardiorenal SyndromeDocument89 pagesCardiorenal SyndromeGabriyah HamzahNo ratings yet
- Att CKD Oct04Document24 pagesAtt CKD Oct04A9 El-EbidiNo ratings yet
- 0800-0840 AKI Nephrology Review Internist2023 2Document58 pages0800-0840 AKI Nephrology Review Internist2023 2Jay Kittichoke PipatdumkoengNo ratings yet
- 16LEC 09b KD The Role of Echo Concise F Pres 021716 BunyiDocument57 pages16LEC 09b KD The Role of Echo Concise F Pres 021716 Bunyiriz04_fortitudessa5178No ratings yet
- Chronic Kidney DiseaseDocument42 pagesChronic Kidney DiseaseLeta GemechuNo ratings yet
- Sickle Cell Topic DiscussionDocument22 pagesSickle Cell Topic Discussionapi-647244341No ratings yet
- Case Presentation: K/Cof: o HTN o Cerebral Aneurysm S/P Clipping On 1992. o CKD Stage 5Document74 pagesCase Presentation: K/Cof: o HTN o Cerebral Aneurysm S/P Clipping On 1992. o CKD Stage 5Thea DinoNo ratings yet
- Vdocument - in - File Kidney DiseaseDocument52 pagesVdocument - in - File Kidney DiseasedfsdsfsdNo ratings yet
- Renin-Angiotensin System Inhibition in Advanced CKDDocument35 pagesRenin-Angiotensin System Inhibition in Advanced CKDbokobokobokanNo ratings yet
- Continuous Ambulatory Peritoneal Dialysis in Diabetic PatientsDocument6 pagesContinuous Ambulatory Peritoneal Dialysis in Diabetic PatientsAjeng SuparwiNo ratings yet
- A Comprehensive Approach To Kidney Disease and Hypertension: Pawang Hazwan Unit Ginjal Dan Hipertensi Ilmu Penyakit DalamDocument47 pagesA Comprehensive Approach To Kidney Disease and Hypertension: Pawang Hazwan Unit Ginjal Dan Hipertensi Ilmu Penyakit DalamMIsbahNo ratings yet
- Gastrointestinal Bleeding: Rajeev Jain, M.DDocument51 pagesGastrointestinal Bleeding: Rajeev Jain, M.DNovita AnjaniNo ratings yet
- Ananya Deb - 18IUT0290004 - PPTDocument16 pagesAnanya Deb - 18IUT0290004 - PPTsubankar NagNo ratings yet
- 2020 Article 390Document2 pages2020 Article 390Riswanto RuslanNo ratings yet
- Problems 1Document6 pagesProblems 1Russel BarquinNo ratings yet
- ST Patricks School Prelim 2021 A MathDocument67 pagesST Patricks School Prelim 2021 A MathFadly RamliNo ratings yet
- Training ReportDocument16 pagesTraining ReportJay MavaniNo ratings yet
- Find Funding: Region or Country Funder (E.g. World Bank, DFID) Topic (E.g. Water & Sanitation)Document5 pagesFind Funding: Region or Country Funder (E.g. World Bank, DFID) Topic (E.g. Water & Sanitation)Bilel MarkosNo ratings yet
- Sintering Process of MagnetsDocument3 pagesSintering Process of MagnetsSAMIT JAINNo ratings yet
- Straegic Issues of Resource Allocation: A Case of Jet AirwaysDocument8 pagesStraegic Issues of Resource Allocation: A Case of Jet AirwaysnanditaNo ratings yet
- Team-1 Module 2 Practice-ProblemsDocument10 pagesTeam-1 Module 2 Practice-ProblemsMay May MagluyanNo ratings yet
- gp30mpc 150Document27 pagesgp30mpc 150locomotoras.slpNo ratings yet
- Activities Unit 4 Lesson 8-10Document13 pagesActivities Unit 4 Lesson 8-10Raven Ann Trinchera PerezNo ratings yet
- Jurnal Resti: Implementasi Algoritma A-Star Untuk Pencarian Ruteterdekat Titik Shelter Evakuasi TsunamiDocument6 pagesJurnal Resti: Implementasi Algoritma A-Star Untuk Pencarian Ruteterdekat Titik Shelter Evakuasi Tsunamipinkyboy79No ratings yet
- Operation Management CHP 1 5Document82 pagesOperation Management CHP 1 5Games FunNo ratings yet
- Dark Matter: Episode #101Document57 pagesDark Matter: Episode #101Santiago Buitrago BeltranNo ratings yet
- SOD882 / SOD923 / 0402 Board Adapter For PrototypingDocument2 pagesSOD882 / SOD923 / 0402 Board Adapter For Prototypingteix9360No ratings yet
- Labor Law Bar Exam 2012 ResearchDocument9 pagesLabor Law Bar Exam 2012 ResearchMalaybalaycity TiktokchallengeNo ratings yet
- Lecture 1 - Information Systems Auditing Overview and MethodologiesDocument65 pagesLecture 1 - Information Systems Auditing Overview and MethodologieskamuturiNo ratings yet
- Brand Awareness Effects On Consumer Decision Making For A Common, Repeat Purchase Product:: A ReplicationDocument12 pagesBrand Awareness Effects On Consumer Decision Making For A Common, Repeat Purchase Product:: A ReplicationSanjana SamarasingheNo ratings yet
- Microprocessor: HCMC, 08/2022Document44 pagesMicroprocessor: HCMC, 08/2022loi DuongNo ratings yet
- Earl Bryan M. Apale: Personal Portfolio)Document7 pagesEarl Bryan M. Apale: Personal Portfolio)Kilk SueNo ratings yet
- NI Multisim TutorialsDocument9 pagesNI Multisim Tutorials322399mk7086No ratings yet
- 32 Bit Multiplication and Division ALU Design Based On RISC StructureDocument4 pages32 Bit Multiplication and Division ALU Design Based On RISC StructureVishnu Kumar NadarNo ratings yet
- PUN Hlaing, Hsu Yadanar AungDocument2 pagesPUN Hlaing, Hsu Yadanar AungHsu Yadanar AungNo ratings yet
- D60 Line Distance Relay: Instruction ManualDocument442 pagesD60 Line Distance Relay: Instruction ManualyaneiroNo ratings yet
- Cisco IE 4000 InstallationDocument44 pagesCisco IE 4000 Installationeabrodriguez3116No ratings yet