You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Kiss Your Dentist GoodbyeDocument155 pagesKiss Your Dentist GoodbyeAmbrose66100% (4)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Talent-Olympiad 4 Science SampleDocument13 pagesTalent-Olympiad 4 Science Sampleshweta051100% (3)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Dental FluorosisDocument70 pagesDental Fluorosiskaran89No ratings yet
- Hpat Ireland Practice TestDocument81 pagesHpat Ireland Practice TestBrian Maloney100% (1)
- 2006 Asda ExamDocument9 pages2006 Asda ExamJon Haynie100% (2)
- Amelogenesis ImperfectaDocument4 pagesAmelogenesis Imperfectamirfanulhaq100% (1)
- Dental Science Dental Radiography Syllabus Hilary Term 2019/20 Fridays 9am-11amDocument4 pagesDental Science Dental Radiography Syllabus Hilary Term 2019/20 Fridays 9am-11amBrian MaloneyNo ratings yet
- Public Health, Health and LifestyleDocument149 pagesPublic Health, Health and LifestyleBrian MaloneyNo ratings yet
- Access and Root Morphology 2020Document19 pagesAccess and Root Morphology 2020Brian MaloneyNo ratings yet
- Untitled DocumentDocument3 pagesUntitled DocumentBrian MaloneyNo ratings yet
- Draft Final Y3 Specific Handbook 2020-2021Document48 pagesDraft Final Y3 Specific Handbook 2020-2021Brian MaloneyNo ratings yet
- Endodontic Core Course 2 / 3 Year B.Dent - Sc. Lab & Lecture ScheduleDocument12 pagesEndodontic Core Course 2 / 3 Year B.Dent - Sc. Lab & Lecture ScheduleBrian MaloneyNo ratings yet
- Untitled DocumentDocument3 pagesUntitled DocumentBrian MaloneyNo ratings yet
- Atypical Facial Pain Clinical Considerations and DDocument5 pagesAtypical Facial Pain Clinical Considerations and DBrian MaloneyNo ratings yet
- Untitled DocumentDocument3 pagesUntitled DocumentBrian MaloneyNo ratings yet
- Untitled DocumentDocument3 pagesUntitled DocumentBrian MaloneyNo ratings yet
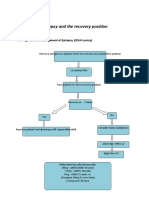
- Epilepsy Recovery Period - Second YrDocument3 pagesEpilepsy Recovery Period - Second YrBrian MaloneyNo ratings yet
- Untitled DocumentDocument3 pagesUntitled DocumentBrian MaloneyNo ratings yet
- Anaphylaxis - Second YearDocument3 pagesAnaphylaxis - Second YearBrian MaloneyNo ratings yet
- Light, Spectroscopy and Metal Complexes 2016 (No Recording)Document18 pagesLight, Spectroscopy and Metal Complexes 2016 (No Recording)Brian MaloneyNo ratings yet
- Developmental Anomlies, Age Changes of TeethDocument61 pagesDevelopmental Anomlies, Age Changes of TeethsethupathiNo ratings yet
- FluorideDocument50 pagesFluoriderajshreeNo ratings yet
- Cariology-The Susceptible Tooth 9Document106 pagesCariology-The Susceptible Tooth 9Free PsPlusNo ratings yet
- 1 - Methods of Measuring Dental FluorosisDocument5 pages1 - Methods of Measuring Dental FluorosisJehad Ali Al-ammariNo ratings yet
- Pedo Case 2Document5 pagesPedo Case 2Aditya MalhotraNo ratings yet
- Diseases of Oral Cavity, Salivary Glands and Jaws (K00-K14) : Search (Advanced Search)Document13 pagesDiseases of Oral Cavity, Salivary Glands and Jaws (K00-K14) : Search (Advanced Search)Ria MarthantiNo ratings yet
- L1 Pediatric Operative Dentistry 1 18-11-21Document28 pagesL1 Pediatric Operative Dentistry 1 18-11-21Ju JuNo ratings yet
- New Microsoft Office Word DocumentDocument3 pagesNew Microsoft Office Word DocumentMohammad ElwirNo ratings yet
- 8 Benefits of Veneers: 1. Simple and EasyDocument3 pages8 Benefits of Veneers: 1. Simple and EasyJosline MuriikiNo ratings yet
- Adhesive Systems in Restorative DentistryDocument6 pagesAdhesive Systems in Restorative DentistryStoian SimonaNo ratings yet
- 2016 Magne Fatigue Resistance and Crack Propensity of Novel Super Closed SandwichDocument17 pages2016 Magne Fatigue Resistance and Crack Propensity of Novel Super Closed Sandwichmaroun ghalebNo ratings yet
- Twin StudiesDocument219 pagesTwin StudiesUniversity of Adelaide PressNo ratings yet
- PM9 Working-Instructions 09Document48 pagesPM9 Working-Instructions 09Alex BurdeNo ratings yet
- Effect of Sterilisation Methods On The Structural Integrity of Artificial Enamel Caries For Intra-Oral Cariogenicity TestsDocument4 pagesEffect of Sterilisation Methods On The Structural Integrity of Artificial Enamel Caries For Intra-Oral Cariogenicity Testsiftita almunirNo ratings yet
- Anatomic Anomalies - LectureDocument10 pagesAnatomic Anomalies - LectureKhalid BhatNo ratings yet
- All Ceramic Cementation A Key To Successful RestorationDocument9 pagesAll Ceramic Cementation A Key To Successful RestorationJUDITH ESTHER HIGUERA MESANo ratings yet
- CLASS II Cavity PreparationDocument10 pagesCLASS II Cavity PreparationNguyễn Huy LongNo ratings yet
- Learning Module - Chapter-6 - Our Teeth - Question and Answers - Grade IVDocument9 pagesLearning Module - Chapter-6 - Our Teeth - Question and Answers - Grade IVankeetaNo ratings yet
- An Overview of Oral TissuesDocument4 pagesAn Overview of Oral TissuesRenukaChauveNo ratings yet
- Tooth Discoloration: DR Bindu Kumari (BDS)Document32 pagesTooth Discoloration: DR Bindu Kumari (BDS)محمد العراقيNo ratings yet
- School Age ReviewerDocument10 pagesSchool Age ReviewerHazel Ann MolinoNo ratings yet
- Assignment No 1 For 4 Year: Nder Upervision ofDocument29 pagesAssignment No 1 For 4 Year: Nder Upervision ofMustafa ShakerNo ratings yet
- Topic 7. X-Ray, Luminescent and Transilluminating Diagnostics: The Indication ToDocument2 pagesTopic 7. X-Ray, Luminescent and Transilluminating Diagnostics: The Indication ToHERO RescueNo ratings yet
- Anatomy and Physiology MouthDocument4 pagesAnatomy and Physiology MouthAndrew BimbusNo ratings yet
- Classification of Veneer PreparationsDocument11 pagesClassification of Veneer PreparationsVinisha Vipin SharmaNo ratings yet