You might also like
- Atypical Facial PainDocument5 pagesAtypical Facial PainRenju KuriakoseNo ratings yet
- Chronic Idiopathic Orofacial Pain I What Is The EvDocument3 pagesChronic Idiopathic Orofacial Pain I What Is The EvAmandaNovrianNo ratings yet
- Orofacial PainDocument7 pagesOrofacial PainAkram AlsharaeeNo ratings yet
- Chronic Facial Pain Guide: Causes, Symptoms & TreatmentsDocument5 pagesChronic Facial Pain Guide: Causes, Symptoms & TreatmentsdamarstationNo ratings yet
- Atypical Facial Pain and Atypical Odontalgia: A Concise ReviewDocument4 pagesAtypical Facial Pain and Atypical Odontalgia: A Concise ReviewAulia ZahroNo ratings yet
- EAOM HandbookDocument249 pagesEAOM HandbookmadhaNo ratings yet
- Phantom Tooth PainDocument31 pagesPhantom Tooth PainMuchlis Fauzi ENo ratings yet
- Facial Presentations of Primary Headache DisordersDocument6 pagesFacial Presentations of Primary Headache DisordersEmmanuel AguilarNo ratings yet
- Erratum IxDocument3 pagesErratum IxKranti PrajapatiNo ratings yet
- Chronic Orofacial PainDocument14 pagesChronic Orofacial PainStra LettNo ratings yet
- 1129-2377-14-37Document10 pages1129-2377-14-37Tatiana AlapeNo ratings yet
- Orofacialpain:: A PrimerDocument10 pagesOrofacialpain:: A Primeranon_768201406No ratings yet
- Orofacial pain daignosis and managementDocument4 pagesOrofacial pain daignosis and managementsm tamNo ratings yet
- Jurnal - Relief of PainDocument6 pagesJurnal - Relief of PainChandra NepaNo ratings yet
- Differential Diagnosis of Facial Pain: Jean SDocument4 pagesDifferential Diagnosis of Facial Pain: Jean SIgnatius Adhi AkuntantoNo ratings yet
- Chronic Orofacial Pain: Burning Mouth Syndrome and Other Neuropathic DisordersDocument28 pagesChronic Orofacial Pain: Burning Mouth Syndrome and Other Neuropathic DisordersGeethanjali SadasivamNo ratings yet
- AN C F P: EW Lassification For Acial AINDocument4 pagesAN C F P: EW Lassification For Acial AINAkmal Niam FirdausiNo ratings yet
- Halpern 2016Document25 pagesHalpern 2016SAYDE ILEANA NAJERA DOMINGUEZNo ratings yet
- Bell'S Palsy: Villanueva, Relyssa Ashley L. BSNDocument6 pagesBell'S Palsy: Villanueva, Relyssa Ashley L. BSNAshley VillanuevaNo ratings yet
- Lonked To Page 26 Acute Orofacial PainDocument10 pagesLonked To Page 26 Acute Orofacial PainguhanderNo ratings yet
- PIIS0007091217329720Document10 pagesPIIS0007091217329720Eva Nina MagdalencNo ratings yet
- Atypical Odontalgia Current Knowledge and Implications For Diagnosis and ManagementDocument5 pagesAtypical Odontalgia Current Knowledge and Implications For Diagnosis and ManagementIma ShofyaNo ratings yet
- Diagnosis Tolosa HuntDocument7 pagesDiagnosis Tolosa HuntHedy AngelineNo ratings yet
- Headache+Medicine,+v 3,+n 2,+p 76-87,+apr MayJun +2012Document12 pagesHeadache+Medicine,+v 3,+n 2,+p 76-87,+apr MayJun +2012dvdbergamascoNo ratings yet
- Atypical OdontalgiaDocument5 pagesAtypical OdontalgiaMaria Putri NasutionNo ratings yet
- Applsci 12 11026Document3 pagesApplsci 12 11026كرم الباريNo ratings yet
- Cephalalgia ReviewDocument25 pagesCephalalgia ReviewApostolos T.No ratings yet
- PMT 2018 0061Document4 pagesPMT 2018 0061jose perezNo ratings yet
- Differential Diagnosis For Orofacial Pain, Including Sinusitis, TMD, Trigeminal NeuralgiaDocument11 pagesDifferential Diagnosis For Orofacial Pain, Including Sinusitis, TMD, Trigeminal NeuralgialyraNo ratings yet
- H. Gremillion-Temporomandibular Disorders and Orafacial Pain, An Issue of Dental Clinics (The Clinics - Dentistry) - Saunders (2007) PDFDocument274 pagesH. Gremillion-Temporomandibular Disorders and Orafacial Pain, An Issue of Dental Clinics (The Clinics - Dentistry) - Saunders (2007) PDFSamuel Flores CalderonNo ratings yet
- 31 Penodynia-HosthotaADocument2 pages31 Penodynia-HosthotaAMarius CiobotaruNo ratings yet
- Rhinogenic Headache: A Controversial Headache TypeDocument10 pagesRhinogenic Headache: A Controversial Headache TypealbertrianthoNo ratings yet
- Mismanagement of Dentoalveolar PainDocument7 pagesMismanagement of Dentoalveolar PainEmily AgueroNo ratings yet
- Fibromyalgia PDFDocument10 pagesFibromyalgia PDFRuan VerzosaNo ratings yet
- Ijcpd 13 196Document3 pagesIjcpd 13 196renianggrainiNo ratings yet
- Jurnal TinitusDocument14 pagesJurnal TinitusAndriyani YaniNo ratings yet
- Eng 1201 Researched Argument PaperDocument10 pagesEng 1201 Researched Argument Paperapi-548399191No ratings yet
- OPERATORIA. Henry A. Gremillion Multidisciplinary Diagnosis and Management of Orofacial PainDocument13 pagesOPERATORIA. Henry A. Gremillion Multidisciplinary Diagnosis and Management of Orofacial PainKenigal14No ratings yet
- HHS Public Access: Chronic Orofacial Pain: Burning Mouth Syndrome and Other Neuropathic DisordersDocument30 pagesHHS Public Access: Chronic Orofacial Pain: Burning Mouth Syndrome and Other Neuropathic DisordersvitasepfinaNo ratings yet
- Clinical Reasoning: A Misdiagnosis of Atypical Trigeminal NeuralgiaDocument9 pagesClinical Reasoning: A Misdiagnosis of Atypical Trigeminal NeuralgiaNisha SharmaNo ratings yet
- Acupuncture - MeniereDocument4 pagesAcupuncture - MeniereTinnitus Man IndonesiaNo ratings yet
- CX + Anatomia + Trigemino + Neuralgia + OclusionDocument5 pagesCX + Anatomia + Trigemino + Neuralgia + OclusionJuan Pablo Mejia BarbosaNo ratings yet
- Misdiagnosed Odontogenic Headache: Case Report and Review of LiteratureDocument2 pagesMisdiagnosed Odontogenic Headache: Case Report and Review of LiteratureAtul DwivediNo ratings yet
- Chronic Sinusitis: A Major Perpetuating Factor?: by Devin J. StarlanylDocument7 pagesChronic Sinusitis: A Major Perpetuating Factor?: by Devin J. StarlanylRiri Ayusa AsriNo ratings yet
- Drugs For Pain ManagementDocument9 pagesDrugs For Pain ManagementbabukanchaNo ratings yet
- Review of Cervical Radiculopathy Causes, Diagnosis and TreatmentDocument8 pagesReview of Cervical Radiculopathy Causes, Diagnosis and TreatmentRenaldiPrimaSaputraNo ratings yet
- 2011 Article 9218 PDFDocument8 pages2011 Article 9218 PDFAgnesya GunawanNo ratings yet
- Pain Definition 1979Document6 pagesPain Definition 1979Hossam BarghashNo ratings yet
- Headache: Paul G. Mathew, M.D., and Ivan Garza, M.DDocument13 pagesHeadache: Paul G. Mathew, M.D., and Ivan Garza, M.DCarlosErnestoMoralesNo ratings yet
- LBP - Dr. Dessy Sp.sDocument77 pagesLBP - Dr. Dessy Sp.srahmadsyahNo ratings yet
- Menieres DiseaseDocument6 pagesMenieres Diseasecceng06No ratings yet
- Facial Pain PDFDocument4 pagesFacial Pain PDFSuprit SnNo ratings yet
- Mandibular Dysfunction and Cranial Pain SyndromesDocument11 pagesMandibular Dysfunction and Cranial Pain SyndromesGuoyiNo ratings yet
- The Pharmacological Management of Vertigo in Meniere DiseaseDocument12 pagesThe Pharmacological Management of Vertigo in Meniere DiseasePablo Sebastián SaezNo ratings yet
- Management of Orofacial PainDocument12 pagesManagement of Orofacial Painhzg973No ratings yet
- ConditionMonograph MenieresDiseaseFINALDocument13 pagesConditionMonograph MenieresDiseaseFINALDeviNo ratings yet
- Bell's Palsy EbnDocument48 pagesBell's Palsy EbnClara Maey GarciaNo ratings yet
- Endodontic Course TitleDocument12 pagesEndodontic Course TitleBrian MaloneyNo ratings yet
- Epidemiology Second YearDocument53 pagesEpidemiology Second YearBrian MaloneyNo ratings yet
- Dental Radiography SyllabusDocument4 pagesDental Radiography SyllabusBrian MaloneyNo ratings yet
- Public Health, Health and LifestyleDocument149 pagesPublic Health, Health and LifestyleBrian MaloneyNo ratings yet
- B13 - Human Diseases IIDocument32 pagesB13 - Human Diseases IIBrian MaloneyNo ratings yet
- Atomic Theory, Dental Science, Sep 2016Document27 pagesAtomic Theory, Dental Science, Sep 2016Brian MaloneyNo ratings yet
- Access and Root Morphology 2020Document19 pagesAccess and Root Morphology 2020Brian MaloneyNo ratings yet
- Glass Ionomer CementDocument21 pagesGlass Ionomer CementRobins DhakalNo ratings yet
- Draft Final Y3 Specific Handbook 2020-2021Document48 pagesDraft Final Y3 Specific Handbook 2020-2021Brian MaloneyNo ratings yet
- CV Brian Maloney Self-Motivated Creative NumericDocument3 pagesCV Brian Maloney Self-Motivated Creative NumericBrian MaloneyNo ratings yet
- Thermochemistry, Dental Science, 2016 (No Recording)Document19 pagesThermochemistry, Dental Science, 2016 (No Recording)Brian MaloneyNo ratings yet
- Key Concepts in Research EthicsDocument4 pagesKey Concepts in Research EthicsBrian MaloneyNo ratings yet
- Light, Spectroscopy and Metal Complexes 2016 (No Recording)Document18 pagesLight, Spectroscopy and Metal Complexes 2016 (No Recording)Brian MaloneyNo ratings yet
- Untitled DocumentDocument3 pagesUntitled DocumentBrian MaloneyNo ratings yet
- Untitled DocumentDocument3 pagesUntitled DocumentBrian MaloneyNo ratings yet
- Untitled DocumentDocument3 pagesUntitled DocumentBrian MaloneyNo ratings yet
- Untitled DocumentDocument3 pagesUntitled DocumentBrian MaloneyNo ratings yet
- Free Practice TestDocument27 pagesFree Practice TestRazor11111No ratings yet
- VITA 1511 1511E Prothetikleitfaden BA EN V01 Screen en PDFDocument150 pagesVITA 1511 1511E Prothetikleitfaden BA EN V01 Screen en PDF玉麒張No ratings yet
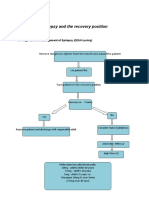
- Epilepsy Recovery Period - Second YrDocument3 pagesEpilepsy Recovery Period - Second YrBrian MaloneyNo ratings yet
- Managing AnaphylaxisDocument3 pagesManaging AnaphylaxisBrian MaloneyNo ratings yet
- Thalassemias An OverviewDocument11 pagesThalassemias An OverviewPippo RudyNo ratings yet
- External Carotid BranchesDocument5 pagesExternal Carotid BranchesBrian MaloneyNo ratings yet
- Vasovagal Second YearDocument2 pagesVasovagal Second YearBrian MaloneyNo ratings yet
- Hpat Ireland Practice Test3Document79 pagesHpat Ireland Practice Test3Brian Maloney85% (13)
- Managing AnaphylaxisDocument3 pagesManaging AnaphylaxisBrian MaloneyNo ratings yet
- Hpat Ireland Practice TestDocument81 pagesHpat Ireland Practice TestBrian Maloney100% (1)
- Atomic Theory, Dental Science, Sep 2016Document27 pagesAtomic Theory, Dental Science, Sep 2016Brian MaloneyNo ratings yet
- Thermochemistry, Dental Science, 2016 (No Recording)Document19 pagesThermochemistry, Dental Science, 2016 (No Recording)Brian MaloneyNo ratings yet
- Teenage Pregnancy Refers To The Adolescent Girls, Usually With in The AgesDocument6 pagesTeenage Pregnancy Refers To The Adolescent Girls, Usually With in The Agesmarina abanNo ratings yet
- 1st Quarter Exam Pe and Health 11Document4 pages1st Quarter Exam Pe and Health 11Irish John GulmaticoNo ratings yet
- 20 Đề tham khảo tuyển sinh vào lớp 10 2022Document87 pages20 Đề tham khảo tuyển sinh vào lớp 10 2022nguyethuhang.hnNo ratings yet
- Effects of Child AbuseDocument38 pagesEffects of Child AbuseChristopher Baccay84% (19)
- Two REBT Therapists and One Client: Ellis TranscriptDocument12 pagesTwo REBT Therapists and One Client: Ellis TranscriptJoaquin OlivaresNo ratings yet
- Guard RailDocument24 pagesGuard RailRESHMANo ratings yet
- Anil's GhostDocument2 pagesAnil's Ghostfaatema0% (1)
- Occlusal Plane Template TechniqueDocument39 pagesOcclusal Plane Template TechniqueREWA KAWADENo ratings yet
- Accomplishment Target For The Month of October C.Y. 2020Document16 pagesAccomplishment Target For The Month of October C.Y. 2020jamesdigolNo ratings yet
- Biodata Peneliti Utama: Rumah Sakit Umum Pusat Dr. Hasan Sadikin BandungDocument2 pagesBiodata Peneliti Utama: Rumah Sakit Umum Pusat Dr. Hasan Sadikin BandungAdriel BenedictNo ratings yet
- Myles Baker - Student Guide CHPT Test 3Document2 pagesMyles Baker - Student Guide CHPT Test 3JJ RealbayNo ratings yet
- Management: Fourteenth EditionDocument46 pagesManagement: Fourteenth EditionAmjad J AliNo ratings yet
- ItDocument4 pagesItNguyễn Duy HuânNo ratings yet
- Chapter 1Document2 pagesChapter 1longaitiNo ratings yet
- Safety Data Sheet: Butyrylcholinesterase Inhibitor Screening Kit (Colorimetric)Document6 pagesSafety Data Sheet: Butyrylcholinesterase Inhibitor Screening Kit (Colorimetric)Verliyanti BastariNo ratings yet
- Reducing AgeismDocument2 pagesReducing AgeismAntónio LealNo ratings yet
- AGREE II Scoring TemplateDocument7 pagesAGREE II Scoring TemplateBasitNo ratings yet
- 4.1.10 Practice Grammar FeedbackDocument10 pages4.1.10 Practice Grammar FeedbackbaileyNo ratings yet
- Immuno GlowDocument11 pagesImmuno GlowNoly ClaveringNo ratings yet
- Cbse Class 12 English Core Sample Paper Term 2Document6 pagesCbse Class 12 English Core Sample Paper Term 2Harender TanwarNo ratings yet
- 03 - Neurotoxicity in OncologyDocument17 pages03 - Neurotoxicity in OncologygorklanNo ratings yet
- HS ConsultantDocument2 pagesHS Consultantdeeman4yahNo ratings yet
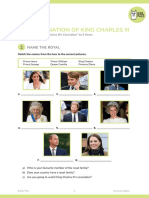
- SV The Coronation of King Charles IIIDocument9 pagesSV The Coronation of King Charles IIIMaria GromovaNo ratings yet
- RA-032739 - MASTER PLUMBER - Lucena - 2-2023Document7 pagesRA-032739 - MASTER PLUMBER - Lucena - 2-2023Bon Opeña GorobaoNo ratings yet
- The Locomotor Module: Removal of MythsDocument8 pagesThe Locomotor Module: Removal of MythsRabia OwaisNo ratings yet
- Biology 2 Macromolecules and NutrientsDocument16 pagesBiology 2 Macromolecules and NutrientsMwendalubi ChiholyongaNo ratings yet
- Yahoo News You Gov Health Poll 3.11.24Document13 pagesYahoo News You Gov Health Poll 3.11.24AndrewNo ratings yet
- Optometry SeniorDocument8 pagesOptometry Seniorapi-504989033No ratings yet
- Diag AutismoDocument12 pagesDiag AutismoSandra Carranza ZavalaNo ratings yet
- Training and DevelopmentDocument2 pagesTraining and DevelopmentBeing Rohit ThakurNo ratings yet