You might also like
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationFrom EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehNo ratings yet
- Tolosa-Hunt Syndrome: A Rare Cause For An Isolated Ocular Nerve Palsy in An Elderly MaleDocument3 pagesTolosa-Hunt Syndrome: A Rare Cause For An Isolated Ocular Nerve Palsy in An Elderly MaleElisabeth TikalakaNo ratings yet
- Austin NeurologyDocument2 pagesAustin NeurologyAustin Publishing GroupNo ratings yet
- Tolosa-Hunt Syndrome: EpidemiologyDocument3 pagesTolosa-Hunt Syndrome: EpidemiologyRiris SihotangNo ratings yet
- Talosa Hunt Syndrome 6Document3 pagesTalosa Hunt Syndrome 6الكاسر الكاسرNo ratings yet
- Clinical Forms of Onset in Tolosa Hunt Syndrome1Document5 pagesClinical Forms of Onset in Tolosa Hunt Syndrome1Ioana CrăciunNo ratings yet
- Bjorl: Mastoiditis and Facial Paralysis As Initial Manifestations of Wegener's GranulomatosisDocument7 pagesBjorl: Mastoiditis and Facial Paralysis As Initial Manifestations of Wegener's GranulomatosismelchiadiNo ratings yet
- Review of Optic Neuritis Treatment TrialDocument5 pagesReview of Optic Neuritis Treatment TrialsatrianiNo ratings yet
- Characteristics of Headache in Relation To The Manifestation of - 2017 - MediciDocument6 pagesCharacteristics of Headache in Relation To The Manifestation of - 2017 - MediciMohammedHajNo ratings yet
- Ssciberras, 17. One-And-A-Half SyndromeDocument5 pagesSsciberras, 17. One-And-A-Half SyndromeDhanyTuasamuNo ratings yet
- Blue Book 2011Document222 pagesBlue Book 2011ashokNo ratings yet
- Edlow 2018Document15 pagesEdlow 2018arianaNo ratings yet
- Presentasi Kasus Sudden Deafness Dhana 2017Document9 pagesPresentasi Kasus Sudden Deafness Dhana 2017Pradhana FwNo ratings yet
- Epileptic Disorders - 2021 - Leibetseder - How To Distinguish Seizures From Non Epileptic ManifestationsDocument23 pagesEpileptic Disorders - 2021 - Leibetseder - How To Distinguish Seizures From Non Epileptic ManifestationsFranklin SierraNo ratings yet
- Diagnosis of Multiple Sclerosis Progress and ChallengesDocument11 pagesDiagnosis of Multiple Sclerosis Progress and Challengessarawu9911No ratings yet
- Tolosa Hunt SyndromeDocument5 pagesTolosa Hunt SyndromeAanisah Ikbaar SayyidahNo ratings yet
- Journal of Neuroimmunology: SciencedirectDocument3 pagesJournal of Neuroimmunology: SciencedirectGrupo 3113 Siglo XXINo ratings yet
- Thijs 2019Document13 pagesThijs 2019Priska CrisnandaNo ratings yet
- Tuli Mnedadak ncbiDocument6 pagesTuli Mnedadak ncbiMiss AmyNo ratings yet
- Work Stress Induced CSCDocument15 pagesWork Stress Induced CSCVincent Rooroh0% (1)
- Acute Disseminated Encephalomyelitis After Rabies Vaccination: One Case ReportDocument4 pagesAcute Disseminated Encephalomyelitis After Rabies Vaccination: One Case ReportIJAR JOURNALNo ratings yet
- ACTHIV29Document1 pageACTHIV29Drashua AshuaNo ratings yet
- Wa0007Document17 pagesWa0007Eko WidodoNo ratings yet
- Complex Regional Pain Syndrome Type 1 in A Pediatric Patient Case ReportDocument4 pagesComplex Regional Pain Syndrome Type 1 in A Pediatric Patient Case ReportBilly Giovanni MantuNo ratings yet
- EFNS-guideline ALS PDFDocument22 pagesEFNS-guideline ALS PDFAhmad ShokryNo ratings yet
- Optic NeuritisDocument12 pagesOptic NeuritisScerbatiuc CristinaNo ratings yet
- DTSCH Arztebl Int-114-0354Document10 pagesDTSCH Arztebl Int-114-0354Shafa KhansaNo ratings yet
- Mitsumoto ALS JAMA07Document11 pagesMitsumoto ALS JAMA07abcdefgNo ratings yet
- Epilepsy in AdultsDocument13 pagesEpilepsy in AdultsHellen SantosNo ratings yet
- Toosy Lancet Neurology 2014Document17 pagesToosy Lancet Neurology 2014Dirga Rasyidin LNo ratings yet
- Tolosa Hunt Syndrome Article from 1977 Indian JournalDocument4 pagesTolosa Hunt Syndrome Article from 1977 Indian JournalAyu Sylvia Axx HpNo ratings yet
- Prognosis RHSDocument6 pagesPrognosis RHSDiah HayustiningsihNo ratings yet
- Case ReportDocument3 pagesCase ReportNeilavery WindaNo ratings yet
- Diagnosis and Treatment of Somatoform DisordersDocument12 pagesDiagnosis and Treatment of Somatoform DisordersSURYANo ratings yet
- Epilepsy in Adults - Lancet 2019Document13 pagesEpilepsy in Adults - Lancet 2019samNo ratings yet
- The Outcome of Status Epilepticus and Long-Term Follow-UpDocument8 pagesThe Outcome of Status Epilepticus and Long-Term Follow-UpDicky LesmanaNo ratings yet
- Central Serous Chorioretinopathy Induced by Work StressDocument16 pagesCentral Serous Chorioretinopathy Induced by Work StressVincent RoorohNo ratings yet
- Commentary: The Optic Neuritis Treatment TrialDocument2 pagesCommentary: The Optic Neuritis Treatment TrialEmmanuel Zótico Orellana JiménezNo ratings yet
- HHS Public Access: Chronic Orofacial Pain: Burning Mouth Syndrome and Other Neuropathic DisordersDocument30 pagesHHS Public Access: Chronic Orofacial Pain: Burning Mouth Syndrome and Other Neuropathic DisordersvitasepfinaNo ratings yet
- Kelleher2020 - Occlusal-DysaesthesiaDocument4 pagesKelleher2020 - Occlusal-DysaesthesiabélaNo ratings yet
- Jurnal Dr. PZDocument45 pagesJurnal Dr. PZRwsunbhio PratamaNo ratings yet
- Seminar: Benjamin E Schreiber, Charlotte Agrup, Dorian O Haskard, Linda M LuxonDocument9 pagesSeminar: Benjamin E Schreiber, Charlotte Agrup, Dorian O Haskard, Linda M Luxonmaria_garaveNo ratings yet
- Pain Practice - 2010 - Van Eijs - 16 Complex Regional Pain SyndromeDocument18 pagesPain Practice - 2010 - Van Eijs - 16 Complex Regional Pain SyndromeZuraidaNo ratings yet
- Atypical Odontalgia Current Knowledge and Implications For Diagnosis and ManagementDocument5 pagesAtypical Odontalgia Current Knowledge and Implications For Diagnosis and ManagementIma ShofyaNo ratings yet
- Warfarin, Winter, and Central Serous ChorioretinopathyDocument2 pagesWarfarin, Winter, and Central Serous ChorioretinopathyBOHR International Journal of Current Research in Optometry and Ophthalmology (BIJCROO)No ratings yet
- Neuro Signs InterpretationDocument17 pagesNeuro Signs InterpretationAgatha SharmaNo ratings yet
- Involucrar A Los Pacientes en El TratamientoDocument5 pagesInvolucrar A Los Pacientes en El TratamientoluciaNo ratings yet
- ICHD-II Diagnostic Criteria For Tolosa-Hunt Syndrome in Idiopathic Inflammatory Syndromes of The Orbit And/or The Cavernous SinusDocument9 pagesICHD-II Diagnostic Criteria For Tolosa-Hunt Syndrome in Idiopathic Inflammatory Syndromes of The Orbit And/or The Cavernous SinusRakasiwi GalihNo ratings yet
- Bilateral Facial Nerve Palsy: Challenges in Diagnosis: Case ReportDocument3 pagesBilateral Facial Nerve Palsy: Challenges in Diagnosis: Case ReportPutri YunandaNo ratings yet
- 10 - Tumefactive Multiple Sclerosis, A RareDocument7 pages10 - Tumefactive Multiple Sclerosis, A RareHenry DanielNo ratings yet
- Red Eye: A Guide For Non-Specialists: MedicineDocument14 pagesRed Eye: A Guide For Non-Specialists: MedicineFapuw Parawansa100% (1)
- Jurnal MS UPNVJ 2020Document6 pagesJurnal MS UPNVJ 2020Latifah AndiniNo ratings yet
- Epilepsy: Bassel F. Shneker, MD, and Nathan B. Fountain, MDDocument53 pagesEpilepsy: Bassel F. Shneker, MD, and Nathan B. Fountain, MDDiane Mx100% (1)
- Seminar: Solomon L Moshé, Emilio Perucca, Philippe Ryvlin, Torbjörn TomsonDocument15 pagesSeminar: Solomon L Moshé, Emilio Perucca, Philippe Ryvlin, Torbjörn TomsonsriworoNo ratings yet
- Unilateral Eye Pain and Paralysis ExplainedDocument10 pagesUnilateral Eye Pain and Paralysis ExplainedRoxana StanciuNo ratings yet
- Tolosa Hunt Syndrome) - Ophthalmology Dept. Getafe University Hospital. JavierDocument5 pagesTolosa Hunt Syndrome) - Ophthalmology Dept. Getafe University Hospital. JavierNISAURRAHMANo ratings yet
- Algoritmo diagnostico de la ceguera monocular en una paciente con neurosarcoidosisDocument8 pagesAlgoritmo diagnostico de la ceguera monocular en una paciente con neurosarcoidosisFarid Santiago Abedrabbo LombeydaNo ratings yet
- Acute Hypotonia in An Infant (2017)Document3 pagesAcute Hypotonia in An Infant (2017)nikos.alexandrNo ratings yet
- From First Symptoms To Diagnosis: Initial Clinical Presentation of Primary Brain TumorsDocument7 pagesFrom First Symptoms To Diagnosis: Initial Clinical Presentation of Primary Brain TumorsMohammad AamirNo ratings yet
- Neuroretinitis Syphilis in Human Immunodeficiency Virus-Infected PatientDocument6 pagesNeuroretinitis Syphilis in Human Immunodeficiency Virus-Infected PatientAnindya AgrasidiNo ratings yet
- DocumentDocument10 pagesDocumentDewintaNo ratings yet
- FdeDocument9 pagesFdenovera wardaliaNo ratings yet
- Diagnosis of Multiple Sclerosis - 2017 Revisions of McDonald PDFDocument13 pagesDiagnosis of Multiple Sclerosis - 2017 Revisions of McDonald PDFricky rdnNo ratings yet
- Diagnosis of Multiple Sclerosis - 2017 Revisions of McDonald PDFDocument13 pagesDiagnosis of Multiple Sclerosis - 2017 Revisions of McDonald PDFricky rdnNo ratings yet
- Pain Worksheet, donebyJiriesGharib, To Add Together To OthersDocument5 pagesPain Worksheet, donebyJiriesGharib, To Add Together To OthersFernando HerreraNo ratings yet
- Phocomelia: A Case Study: March 2014Document3 pagesPhocomelia: A Case Study: March 2014Nexi anessaNo ratings yet
- Common Lab Tests & Their Use in Diagnosis & Treatment PDFDocument17 pagesCommon Lab Tests & Their Use in Diagnosis & Treatment PDFChAwaisNo ratings yet
- Large Animal Internal DiseasesDocument4 pagesLarge Animal Internal Diseasesiin AgustinaNo ratings yet
- Local Treatment With A Polycarbophil-Based Cream in Postmenopausal Women With Genitourinary Syndrome of MenopauseDocument6 pagesLocal Treatment With A Polycarbophil-Based Cream in Postmenopausal Women With Genitourinary Syndrome of MenopauseBerry BancinNo ratings yet
- Musculoskeletal Examination Under GraduatesDocument98 pagesMusculoskeletal Examination Under GraduatesEsraa SalemNo ratings yet
- Streptococcus PyogenesDocument5 pagesStreptococcus PyogenesKrutika SNo ratings yet
- Fibrinolytic DisordersDocument29 pagesFibrinolytic DisordersChelly JimenoNo ratings yet
- Nursing care analysis of diabetic retinopathyDocument8 pagesNursing care analysis of diabetic retinopathyDonnabell DayudayNo ratings yet
- Material 3 - Acute Kidney Injury in Children - Fauziah Rudhiati, MKep., Sp. Kep - An PDFDocument21 pagesMaterial 3 - Acute Kidney Injury in Children - Fauziah Rudhiati, MKep., Sp. Kep - An PDFINTAN MADULARANo ratings yet
- Neonatal LupusDocument19 pagesNeonatal Lupusyogeshraval368No ratings yet
- Neurological History and Physical ExaminationDocument21 pagesNeurological History and Physical Examinationg3murtulu100% (1)
- DKA Study GroupDocument24 pagesDKA Study GroupAqila MumtazNo ratings yet
- Jurnal Polip ServiksDocument5 pagesJurnal Polip ServiksSilvi IndahrhaNo ratings yet
- Analgesic Agents: Maya Ganda Ratna Department of Pharmacology and Pharmacy Faculty of Medicine - Lampung UniversityDocument46 pagesAnalgesic Agents: Maya Ganda Ratna Department of Pharmacology and Pharmacy Faculty of Medicine - Lampung UniversityMuhammad GilangNo ratings yet
- Prevention of Diabetic Foot Ulcers The Bottlenecks in The PathwayDocument3 pagesPrevention of Diabetic Foot Ulcers The Bottlenecks in The PathwayreuniNo ratings yet
- General Surgery: (Gallbladder Disease)Document1 pageGeneral Surgery: (Gallbladder Disease)Matt100% (1)
- Herpetic Gingivostomatitis in Young ChildrenDocument8 pagesHerpetic Gingivostomatitis in Young ChildrenEunike NabasaNo ratings yet
- Pharmacokinetic-Pharmacodynamic Crisis in The Elderly: Ehab S. Eldesoky, MD, PHDDocument11 pagesPharmacokinetic-Pharmacodynamic Crisis in The Elderly: Ehab S. Eldesoky, MD, PHDMonica LucaciuNo ratings yet
- Biological ChemistryDocument28 pagesBiological ChemistryArsilan Aziz LoneNo ratings yet
- Facial Itching and Demodex folliculorumDocument9 pagesFacial Itching and Demodex folliculorumRisky PerdanaNo ratings yet
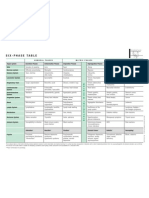
- Six-Phase Table: International Society of HomotoxicologyDocument1 pageSix-Phase Table: International Society of HomotoxicologyPablo Matas SoriaNo ratings yet
- ACUTE AND CHRONIC PHARYNGITIS, ANGINA AND ABSCESSESDocument71 pagesACUTE AND CHRONIC PHARYNGITIS, ANGINA AND ABSCESSESsimi yNo ratings yet
- Miz Mcqs Marking KeyDocument8 pagesMiz Mcqs Marking KeyMich KidNo ratings yet
- Gingival Enlargement - DelDocument64 pagesGingival Enlargement - DeldelsaNo ratings yet
- Semiology 998Document121 pagesSemiology 998Popescu Nicusor100% (1)
- 2 Conversion of Iv To PoDocument27 pages2 Conversion of Iv To PoSreya Sanil100% (1)
- H&PEDocument2 pagesH&PEDanielleNo ratings yet
- Oxigenoterapia Parte 2 Indicaciones y ToxicidadDocument9 pagesOxigenoterapia Parte 2 Indicaciones y ToxicidadyeseyeseprimisNo ratings yet
- Drug Study (Loxapine, Haloperidol)Document5 pagesDrug Study (Loxapine, Haloperidol)kuro hanabusa100% (2)