You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Neurology Notes - PassmedicineDocument71 pagesNeurology Notes - PassmedicineMohammad SalehNo ratings yet
- Rhythm P Wave PR Interval QRS Rate Regularity Life Threatening CausesDocument3 pagesRhythm P Wave PR Interval QRS Rate Regularity Life Threatening CausesLedio XhezairiNo ratings yet
- Poster1 Arrhythmia Recognition e PDFDocument1 pagePoster1 Arrhythmia Recognition e PDFPierf-17No ratings yet
- Echotech Reporting Guidelines Version 15Document30 pagesEchotech Reporting Guidelines Version 15AbrahamNo ratings yet
- PASSMEDICINE MCQs-PHARMACOLOGYDocument107 pagesPASSMEDICINE MCQs-PHARMACOLOGYMohammad Saleh100% (1)
- Heart Failure in ChildrenDocument27 pagesHeart Failure in ChildrendenakarinaNo ratings yet
- " An Attempt To Shorten Hospitalization ": Code StrokeDocument56 pages" An Attempt To Shorten Hospitalization ": Code Stroketricia isabella100% (1)
- Coronary Artery Disease (CAD Pathophysiology)Document5 pagesCoronary Artery Disease (CAD Pathophysiology)Akasha Frostmourne100% (4)
- National University of Sciences and Technology (NUST) : Lab ReportDocument7 pagesNational University of Sciences and Technology (NUST) : Lab ReportMohammad Saleh100% (1)
- BJTsDocument30 pagesBJTsMohammad SalehNo ratings yet
- Quran NotesDocument16 pagesQuran NotesMohammad SalehNo ratings yet
- CS-144 Fundamentals of Programming: Project: House Designs Group: 7 M.Haider Bin ArifDocument8 pagesCS-144 Fundamentals of Programming: Project: House Designs Group: 7 M.Haider Bin ArifMohammad SalehNo ratings yet
- ECG InterpretationDocument108 pagesECG InterpretationMohammad SalehNo ratings yet
- National University of Sciences and Technology (NUST) : Lab ReportDocument6 pagesNational University of Sciences and Technology (NUST) : Lab ReportMohammad SalehNo ratings yet
- Compound PendulumDocument7 pagesCompound PendulumMohammad SalehNo ratings yet
- 1) Brinell Hardness Test Machine 2) Steel Ball Intender 3) Microscope 4) Flat Discs With Finished SurfacesDocument2 pages1) Brinell Hardness Test Machine 2) Steel Ball Intender 3) Microscope 4) Flat Discs With Finished SurfacesMohammad SalehNo ratings yet
- MCPS, TranscriptDocument1 pageMCPS, TranscriptMohammad SalehNo ratings yet
- Cambridge International ExaminationDocument1 pageCambridge International ExaminationMohammad SalehNo ratings yet
- Safa 218-00-000 SITE SURVEYDocument11 pagesSafa 218-00-000 SITE SURVEYMohammad SalehNo ratings yet
- Department of Physics, SNS: National University of Science & Technology (NUST) School of Natural Science (SNS)Document5 pagesDepartment of Physics, SNS: National University of Science & Technology (NUST) School of Natural Science (SNS)Mohammad SalehNo ratings yet
- National University of Sciences and Technology (NUST) CS-114 Fundamentals of ProgrammingDocument10 pagesNational University of Sciences and Technology (NUST) CS-114 Fundamentals of ProgrammingMohammad SalehNo ratings yet
- National University of Sciences and Technology (NUST) : Lab ReportDocument10 pagesNational University of Sciences and Technology (NUST) : Lab ReportMohammad SalehNo ratings yet
- 4 5931499803149076504 PDFDocument126 pages4 5931499803149076504 PDFCristianAltunaSotomayorNo ratings yet
- Future Scope and Challenges For Congestive Heart Failure Moving Towards Development of PharmacotherapyDocument47 pagesFuture Scope and Challenges For Congestive Heart Failure Moving Towards Development of PharmacotherapysunhaolanNo ratings yet
- Colchicine in Coronary Artery Disease (NEJM, 2020) PDFDocument10 pagesColchicine in Coronary Artery Disease (NEJM, 2020) PDFthe_leoNo ratings yet
- Pharmacotherapy OF Acute Coronary Syndrome: Girum SebsibeDocument71 pagesPharmacotherapy OF Acute Coronary Syndrome: Girum SebsibeABREHAM BUKULONo ratings yet
- ABC of Clinical Electrocardiography Broad Complex Tachycardia-Part IDocument4 pagesABC of Clinical Electrocardiography Broad Complex Tachycardia-Part IIgnacio Aguilar ValdiviesoNo ratings yet
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDocument15 pagesDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateHartanto SantosoNo ratings yet
- 1 s2.0 S2772930322004367 MainDocument15 pages1 s2.0 S2772930322004367 MainVimal NishadNo ratings yet
- PJBDocument13 pagesPJBAmaliahHarumiKarimNo ratings yet
- Kelompok 15 PBL 2Document26 pagesKelompok 15 PBL 2Riqah Nefiyanti WardanaNo ratings yet
- Congestive Heart Failure - PathophysiologyDocument1 pageCongestive Heart Failure - PathophysiologyPong's Teodoro SalvadorNo ratings yet
- Acynotic Congenital Heart Diseases: FFU May 2020Document14 pagesAcynotic Congenital Heart Diseases: FFU May 2020gibreilNo ratings yet
- SVT With Aberrancy Versus VTDocument5 pagesSVT With Aberrancy Versus VTEdwin MayaNo ratings yet
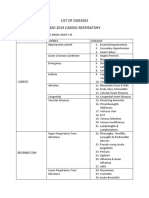
- List of Diseases Imo 2019 Cardio-RespiratoryDocument2 pagesList of Diseases Imo 2019 Cardio-RespiratoryDimas Adjie Yuda MahendraNo ratings yet
- PAVSDMAPCAsDocument3 pagesPAVSDMAPCAsRajesh SharmaNo ratings yet
- Pathophysiology of HTN and CHF Leading To Pleural Effusion Causing Cardiac Tamponade Secondary To PericarditisDocument1 pagePathophysiology of HTN and CHF Leading To Pleural Effusion Causing Cardiac Tamponade Secondary To Pericarditisjake251996No ratings yet
- Mid-Term PresentationDocument18 pagesMid-Term Presentationapi-480918653No ratings yet
- Cardiac DrugsDocument2 pagesCardiac DrugsMhaycelle InsertapilyedohereNo ratings yet
- Ecg in Emergency: Adi SulistyantoDocument41 pagesEcg in Emergency: Adi Sulistyantomech_pilot2203No ratings yet
- Atrial Septal DefectDocument2 pagesAtrial Septal DefectElizabethNo ratings yet
- The ECG in Hypothermia - Osborn WavesDocument2 pagesThe ECG in Hypothermia - Osborn WavesVid MirosevicNo ratings yet
- Daftar Pustaka ImaDocument2 pagesDaftar Pustaka ImaDesrina PungkyNo ratings yet
- Cerebrovascular AccidentDocument12 pagesCerebrovascular AccidentMarvie JOiz AnteNo ratings yet
- Sample PrognosisDocument3 pagesSample PrognosisjudssalangsangNo ratings yet
- Download pdf Acls Study Guide Barbara J Aehlert ebook full chapterDocument53 pagesDownload pdf Acls Study Guide Barbara J Aehlert ebook full chapterivan.stephens123100% (3)