You might also like
- Uworld BiochemistryDocument137 pagesUworld Biochemistryهنادي رازمNo ratings yet
- Nbme 11Document102 pagesNbme 11Mohamed Nabil100% (36)
- Genetics 50qDocument62 pagesGenetics 50qAnonymous 4txA8N8etNo ratings yet
- Genetic DiseasesDocument108 pagesGenetic DiseasesRizki Widya NurNo ratings yet
- Genetic and Pediatric DiseasesDocument88 pagesGenetic and Pediatric DiseasesJaneNo ratings yet
- Medical Triads, Tetrads, and PentadsDocument10 pagesMedical Triads, Tetrads, and PentadsAyessa BandalNo ratings yet
- Pathoma LectureDocument385 pagesPathoma LectureMustafa Thaier Al-Karaghouli91% (22)
- Inborn Errors of MetabolismDocument27 pagesInborn Errors of MetabolismShelyAzradNo ratings yet
- Fast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseFrom EverandFast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseNo ratings yet
- National Geographic USA - 04 2019 PDFDocument153 pagesNational Geographic USA - 04 2019 PDFLightbulb LcNo ratings yet
- Kents Twelve ObservationDocument21 pagesKents Twelve ObservationJR100% (1)
- Hypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Drug StudyDocument5 pagesDrug StudyAika CortesNo ratings yet
- Polyhydramnios 10Document4 pagesPolyhydramnios 10hussain AltaherNo ratings yet
- All Mcqs of CHNDocument115 pagesAll Mcqs of CHNumar khan93% (46)
- Patho. Reviewer On Cellular InjuryDocument21 pagesPatho. Reviewer On Cellular InjurySeff CausapinNo ratings yet
- Fanconi SyndromeDocument9 pagesFanconi SyndromeEmilio AldreteNo ratings yet
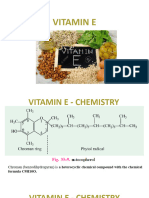
- Vitamin EDocument23 pagesVitamin EffshikaariNo ratings yet
- 1.3 Intracellular AccumulationsDocument52 pages1.3 Intracellular AccumulationsRawa MuhsinNo ratings yet
- Cell InjuryDocument4 pagesCell Injuryrachitagupta1432No ratings yet
- NBME 11 Answers To All Sections 2Document97 pagesNBME 11 Answers To All Sections 2hussainalmusawiNo ratings yet
- I. Intracellular Accumulations of Lipids Fatty ChangeDocument5 pagesI. Intracellular Accumulations of Lipids Fatty ChangeIsak ShatikaNo ratings yet
- UNIMAS Faculty of Medicine and Health Sciences Block 5 Endocrine, Metabolism and Nutrition PBL SummaryDocument7 pagesUNIMAS Faculty of Medicine and Health Sciences Block 5 Endocrine, Metabolism and Nutrition PBL SummaryMuhammad Ilyas AhmadNo ratings yet
- Metabolic Disorders Presentation Group 2Document33 pagesMetabolic Disorders Presentation Group 2Elijah MogoaNo ratings yet
- Ple 2015 Board Review May 2015 Patho OnlyDocument10 pagesPle 2015 Board Review May 2015 Patho OnlyMa Katherina ArellanoNo ratings yet
- Systemic SclerosisDocument36 pagesSystemic SclerosisrgardónNo ratings yet
- Macrocytic Anemia May Be Classified As MegaloblasticDocument5 pagesMacrocytic Anemia May Be Classified As MegaloblasticOjambo FlaviaNo ratings yet
- Vitamin C Deficiency - StatPearls - NCBI BookshelfDocument5 pagesVitamin C Deficiency - StatPearls - NCBI BookshelfJenny BNo ratings yet
- Etiology of Cellular InjuryDocument5 pagesEtiology of Cellular InjuryAFSAL appuNo ratings yet
- Robbins File For AnkiDocument13 pagesRobbins File For Ankiאיתי עוזרNo ratings yet
- Endocrine SystemDocument42 pagesEndocrine SystemBio CheNo ratings yet
- SGD Case: Hematology Weakness: Dizziness: Anorexia: Vomit: Numbness: TinglingingDocument10 pagesSGD Case: Hematology Weakness: Dizziness: Anorexia: Vomit: Numbness: TinglingingEveryday FundayNo ratings yet
- Protein Related Disorders: College of PharmacyDocument37 pagesProtein Related Disorders: College of PharmacyMaureen Chavez KinneyNo ratings yet
- What Is Cystic Fibrosis???Document14 pagesWhat Is Cystic Fibrosis???Naman KulthiaNo ratings yet
- 01 Metabolic Diseases CADocument47 pages01 Metabolic Diseases CAMi PatelNo ratings yet
- Pathology DR - Subh ACD & Megaloblastic Anemia Lec 26: PathogenesisDocument5 pagesPathology DR - Subh ACD & Megaloblastic Anemia Lec 26: PathogenesisS ANo ratings yet
- Intracellular Accumulations: DR - Maha ArafahDocument65 pagesIntracellular Accumulations: DR - Maha Arafahraanja2No ratings yet
- Cellular Injury & AdaptationDocument98 pagesCellular Injury & AdaptationFYMNo ratings yet
- Fat Soluble Vitamin RevisedDocument80 pagesFat Soluble Vitamin RevisedsumitNo ratings yet
- Plugin DisordersDocument3 pagesPlugin DisordersonatkaddNo ratings yet
- Cystic Fibrosis: Navigation SearchDocument15 pagesCystic Fibrosis: Navigation SearchLucyellowOttemoesoeNo ratings yet
- Case Study 6Document14 pagesCase Study 6api-346115799No ratings yet
- Deficiencies of Water Soluble VitaminsDocument20 pagesDeficiencies of Water Soluble Vitaminsbpt2No ratings yet
- IJRPR7994Document6 pagesIJRPR7994rifa iNo ratings yet
- Ms. Tashmera P. Datukali: Mindanao State University Buug Campus - Ipil Extension Sanito, Ipil, Zamboanga Sibugay ProvinceDocument12 pagesMs. Tashmera P. Datukali: Mindanao State University Buug Campus - Ipil Extension Sanito, Ipil, Zamboanga Sibugay Provincesandro2000No ratings yet
- Medecine (English) NORD Complete) Diseases List of Rare DisordersDocument759 pagesMedecine (English) NORD Complete) Diseases List of Rare Disordersyannick100% (2)
- Usmle Step1 Nbme Form 7 Block 1Document24 pagesUsmle Step1 Nbme Form 7 Block 1tejakomminenisNo ratings yet
- 4 Print Fatty Acid Metabo in Born ErrorsDocument35 pages4 Print Fatty Acid Metabo in Born Errorskamalamin2009No ratings yet
- Hypothyroidism MEDSTUDENTS-ENDOCRINOLOGYDocument4 pagesHypothyroidism MEDSTUDENTS-ENDOCRINOLOGYdr,indra SpOGNo ratings yet
- Megaloblastic AnemiasDocument21 pagesMegaloblastic AnemiasDaniel Oviedo ChávezNo ratings yet
- Inborn Error of Metabolism - ايهDocument74 pagesInborn Error of Metabolism - ايهAyaNo ratings yet
- Anaemia in Children by Nsubuga Hamisi: Year 3 MBCHB Facilitated by Dr. Kamugisha Albert Date 29/09/2017Document38 pagesAnaemia in Children by Nsubuga Hamisi: Year 3 MBCHB Facilitated by Dr. Kamugisha Albert Date 29/09/2017NinaNo ratings yet
- AgingDocument12 pagesAgingMasum ShahriarNo ratings yet
- Food & Nutrition Journal: Protein Calorie MalnutritionDocument4 pagesFood & Nutrition Journal: Protein Calorie MalnutritionCamelia NuraNo ratings yet
- Bio NotesDocument24 pagesBio NotesIslam MansourNo ratings yet
- AMYLOIDOSISDocument66 pagesAMYLOIDOSISapi-3856362100% (1)
- Fast Facts: Deficit di piruvato chinasi per pazienti e sostenitori: Una rara malattia genetica che colpisce I globuli rossi Informazioni + assunzione del controllo = migliore risultatoFrom EverandFast Facts: Deficit di piruvato chinasi per pazienti e sostenitori: Una rara malattia genetica che colpisce I globuli rossi Informazioni + assunzione del controllo = migliore risultatoNo ratings yet
- The Metabolic SyndromeFrom EverandThe Metabolic SyndromeChristopher D. ByrneNo ratings yet
- Membrane Lipid Signaling in Aging and Age-Related DiseaseFrom EverandMembrane Lipid Signaling in Aging and Age-Related DiseaseNo ratings yet
- Aspergillus: Dr.D.Bindu Assistant Professor Department of MicrobiologyDocument18 pagesAspergillus: Dr.D.Bindu Assistant Professor Department of Microbiologybindu dhanapalNo ratings yet
- Evaluation of The Febrile Patient A Case-Based Approach: Fevers and Fevers of Unknown OriginDocument97 pagesEvaluation of The Febrile Patient A Case-Based Approach: Fevers and Fevers of Unknown Originkrish vjNo ratings yet
- PICUDocument4 pagesPICUmanisshhaaddNo ratings yet
- Questions and Answer Group 3 "Glaucoma" Nama: Gustin Ibrahim Umamah Kelas: A S1 FARMASI 2017 NIM: 821417021Document13 pagesQuestions and Answer Group 3 "Glaucoma" Nama: Gustin Ibrahim Umamah Kelas: A S1 FARMASI 2017 NIM: 821417021Afni YunitaNo ratings yet
- Epi Lecture 1 Part IIDocument36 pagesEpi Lecture 1 Part IIMowlidAbdirahman Ali madaaleNo ratings yet
- Chapter 27: Alterations of Pulmonary Function Power-Kean Et Al: Huether and Mccance'S Understanding Pathophysiology, Second Canadian EditionDocument13 pagesChapter 27: Alterations of Pulmonary Function Power-Kean Et Al: Huether and Mccance'S Understanding Pathophysiology, Second Canadian EditionmonicaNo ratings yet
- Advocacy in BarangayDocument1 pageAdvocacy in BarangayMJ ValeraNo ratings yet
- Classification of Clinically Significant Bacteria by GenusDocument2 pagesClassification of Clinically Significant Bacteria by GenusSEAN BUINo ratings yet
- Healthcare System in The US Vs France - EditedDocument8 pagesHealthcare System in The US Vs France - EditedMaxine KENo ratings yet
- CPG IP Pneumonia-AdultDocument15 pagesCPG IP Pneumonia-Adultkarthi keyanNo ratings yet
- NYSTAGMUSDocument13 pagesNYSTAGMUSwillemlrouxNo ratings yet
- JESUS DE JESUS, Petitioner, Employees' Compensation Commission, Government Service Insurance System (Philippine National Railways), RespondentsDocument12 pagesJESUS DE JESUS, Petitioner, Employees' Compensation Commission, Government Service Insurance System (Philippine National Railways), RespondentsTiff DizonNo ratings yet
- DR CertificateDocument1 pageDR CertificateSusovan SirNo ratings yet
- Cano-Vindel 2016 Transdiagnostic CBT Vs As UsualDocument16 pagesCano-Vindel 2016 Transdiagnostic CBT Vs As UsualKatrin Gálvez KalliesNo ratings yet
- Landmark Studies in Schizophrenia and Mood Disorders Final PDFDocument46 pagesLandmark Studies in Schizophrenia and Mood Disorders Final PDFSarbartha PramanikNo ratings yet
- Crohns DiseaseDocument21 pagesCrohns DiseaseKasuganti koteshwar raoNo ratings yet
- 5.2.7. Dental Implantation (Situational Tasks)Document2 pages5.2.7. Dental Implantation (Situational Tasks)Tim KurbanovNo ratings yet
- DD DemensiaDocument25 pagesDD DemensiaPutri HarahapNo ratings yet
- Case Scenarios 5Document4 pagesCase Scenarios 5Bianca Mae0% (3)
- Partial Hip Replacement EditedDocument68 pagesPartial Hip Replacement EditedESTHER ROSE ZACALNo ratings yet
- IGNOU Block 3 Unit 1 Epidemiology of Specific Communicable DiseasesDocument9 pagesIGNOU Block 3 Unit 1 Epidemiology of Specific Communicable Diseaseserice.researchNo ratings yet
- BÀI TẬP SS HƠN, SS NHẤT + HOMETOWN+ DISEASESDocument12 pagesBÀI TẬP SS HƠN, SS NHẤT + HOMETOWN+ DISEASESLan AnhNo ratings yet
- Module in Chapter 3Document21 pagesModule in Chapter 3Laiza Mae Autor100% (1)
- Diphtheria: Sabah Mohsin Al-Maamuri MDDocument3 pagesDiphtheria: Sabah Mohsin Al-Maamuri MDAmmar AlnajjarNo ratings yet