You might also like
- Pulmonary HypertensionDocument63 pagesPulmonary HypertensionChrishan Shivanthan100% (4)
- LEGIT 62 Ako 1RST Quarter Exam PDEV 111 1Document23 pagesLEGIT 62 Ako 1RST Quarter Exam PDEV 111 1Mylen Noel Elgincolin Manlapaz50% (2)
- Daily Lesson Plan in English Grade 7 (Quarter 3-Module 5)Document2 pagesDaily Lesson Plan in English Grade 7 (Quarter 3-Module 5)Ramil60% (5)
- Pulmonary HTNDocument59 pagesPulmonary HTNapi-3757039No ratings yet
- HTPAnnals 2005Document12 pagesHTPAnnals 2005api-3703544No ratings yet
- Pulmonary Interstitial/Vascular Involvement: In-Depth Discussion IiDocument12 pagesPulmonary Interstitial/Vascular Involvement: In-Depth Discussion IiAna-Maria IoniţăNo ratings yet
- Management of Pulmonary Hypertension in the ICUDocument52 pagesManagement of Pulmonary Hypertension in the ICUsarsalNo ratings yet
- Pulmonary HypertensionDocument36 pagesPulmonary HypertensionDiana_anca6100% (2)
- 1 s2.0 S1936878X14010122 MainDocument17 pages1 s2.0 S1936878X14010122 MainAnonymous oQtve4oNo ratings yet
- Pulmonary Hypertension - LITFL - CCC CardiologyDocument1 pagePulmonary Hypertension - LITFL - CCC CardiologymyaqanithaNo ratings yet
- Itisnotape: Respiratory Team Teaching BNHH DR Yazeed Abed El Khaleq Respiratory ST4Document28 pagesItisnotape: Respiratory Team Teaching BNHH DR Yazeed Abed El Khaleq Respiratory ST4YazeedNo ratings yet
- RV&PAHDocument24 pagesRV&PAHGiorgi BibilashviliNo ratings yet
- Pulmonary Hypertension Associated With Left-Sided Heart DiseaseDocument13 pagesPulmonary Hypertension Associated With Left-Sided Heart DiseaseIvanes IgorNo ratings yet
- Atow 459 00Document9 pagesAtow 459 00Javier Fernando Cabezas MeloNo ratings yet
- 8) Chronic Cor PulmonaleDocument2 pages8) Chronic Cor PulmonaleAris PaparisNo ratings yet
- Evaluation and Management of Right-SidedDocument65 pagesEvaluation and Management of Right-SidedJevin JameriaNo ratings yet
- 10 1016@j CCL 2020 04 008Document12 pages10 1016@j CCL 2020 04 008Linda Silvana SariNo ratings yet
- Cor Pulmonale ReDocument35 pagesCor Pulmonale ReFabb NelsonNo ratings yet
- Pulmonary Hypertension: and Its Implications For AnaesthesiaDocument31 pagesPulmonary Hypertension: and Its Implications For AnaesthesiaMay LeongNo ratings yet
- Thay Đ I Hình Thái Tăng Áp PH IDocument20 pagesThay Đ I Hình Thái Tăng Áp PH INguyễn Đặng Tường Y2018No ratings yet
- Hipertensión Pulmonar Por Enfermedad VálvulasDocument10 pagesHipertensión Pulmonar Por Enfermedad Válvulasluiserikolivares1390No ratings yet
- Persistent Pulmonary Hypertension of The NewbornDocument6 pagesPersistent Pulmonary Hypertension of The NewbornMarceline GarciaNo ratings yet
- Pulmonary HypertensionDocument15 pagesPulmonary HypertensionChinju CyrilNo ratings yet
- Update On Pulmonary Hypertension and Implications For Solid Organ TransplantationDocument58 pagesUpdate On Pulmonary Hypertension and Implications For Solid Organ TransplantationIrving H Torres LopezNo ratings yet
- Cor Pulmonal and CHDDocument44 pagesCor Pulmonal and CHDamir iksanNo ratings yet
- Cor Pulmonale: Right Heart Failure Due to Lung DiseaseDocument62 pagesCor Pulmonale: Right Heart Failure Due to Lung DiseaseAlbert NixonNo ratings yet
- KP 2.5.5.3 Cor PulmonaleDocument17 pagesKP 2.5.5.3 Cor Pulmonalenurul ramadhiniNo ratings yet
- Pulmonary Artery Hypertension: A Review of Pathophysiology, Symptoms, and Treatment (PAHDocument21 pagesPulmonary Artery Hypertension: A Review of Pathophysiology, Symptoms, and Treatment (PAHAzizi Abd RahmanNo ratings yet
- AJAB CAR Pulmonary HypertensionDocument51 pagesAJAB CAR Pulmonary HypertensionAjabsingh ChoudharyNo ratings yet
- In pregnancy: Heart disease managementDocument47 pagesIn pregnancy: Heart disease managementNATTAPAT SANGKAKULNo ratings yet
- Pulmonary Hypertension: Saurabh Biswas PGT, Dept. of Chest Medicine, CNMCHDocument59 pagesPulmonary Hypertension: Saurabh Biswas PGT, Dept. of Chest Medicine, CNMCHbsaurabh20No ratings yet
- Cardiology Notes by Wasim AhmadDocument28 pagesCardiology Notes by Wasim AhmadAshna moeenNo ratings yet
- Mehlmanmedical Hy PulmonaryDocument31 pagesMehlmanmedical Hy PulmonaryJennifer Ross-ComptisNo ratings yet
- HAP Pulmonar 19Document106 pagesHAP Pulmonar 19jorge corolla montesNo ratings yet
- Pulmonary Hypertension: 1. Identify Pulmonary Hypertension 2. Apply Required Collaborative and Nursing Care PlanDocument14 pagesPulmonary Hypertension: 1. Identify Pulmonary Hypertension 2. Apply Required Collaborative and Nursing Care PlanJeffrey KauvaNo ratings yet
- Management of Cyanotic Child BivinDocument48 pagesManagement of Cyanotic Child BivinChippy BivinNo ratings yet
- Classification and Prognosis of Pulmonary Hypertension in AdultsDocument11 pagesClassification and Prognosis of Pulmonary Hypertension in AdultsIrina MarinNo ratings yet
- Case Report on Primary Pulmonary HypertensionDocument4 pagesCase Report on Primary Pulmonary HypertensionaknbdgNo ratings yet
- Pulmonary HypertensionDocument54 pagesPulmonary HypertensionmendaimashokombaNo ratings yet
- Pulmonary Hypertension: How Should It Be Evaluated? When Is It Important?Document57 pagesPulmonary Hypertension: How Should It Be Evaluated? When Is It Important?prasad8384No ratings yet
- Cyanotic Congenital Heart DiseaseDocument58 pagesCyanotic Congenital Heart Diseasegolden37No ratings yet
- Pulmonary HTNDocument51 pagesPulmonary HTNMuhammad HaekalNo ratings yet
- Hipertensión PulmonarDocument17 pagesHipertensión PulmonarElias Vera RojasNo ratings yet
- Pulmonary Hypertension: A Guide to Pathogenesis, Diagnosis and TreatmentDocument27 pagesPulmonary Hypertension: A Guide to Pathogenesis, Diagnosis and Treatmentantonello picernoNo ratings yet
- Pulmonary Arterial HypertensionDocument16 pagesPulmonary Arterial HypertensionvictorNo ratings yet
- "Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareDocument51 pages"Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareSohil ElfarNo ratings yet
- Pulmonary Embolism PEDocument18 pagesPulmonary Embolism PESafa SalehNo ratings yet
- PH in The ICUDocument10 pagesPH in The ICUSabrinaAyuPutriNo ratings yet
- Pulmonary Embolism: DR Ntambo L.KDocument43 pagesPulmonary Embolism: DR Ntambo L.Khazunga rayfordNo ratings yet
- Approach To The Patient With Shortness of Breath: Colin EdwardsDocument37 pagesApproach To The Patient With Shortness of Breath: Colin EdwardsNur FadzilahNo ratings yet
- Nejmra 2000348Document16 pagesNejmra 2000348Mathew McCarthyNo ratings yet
- Nejm PahDocument16 pagesNejm PahAlexander XavierNo ratings yet
- Pulmonary HypertensionDocument26 pagesPulmonary Hypertensionakoeljames8543No ratings yet
- Respiratory FaillureDocument45 pagesRespiratory FaillureRika AmaliyaNo ratings yet
- Guideline USA 2020Document16 pagesGuideline USA 2020Rodrigo Felipe Albuquerque Paiva de OliveiraNo ratings yet
- Cor Pulmonale - StatPearls - NCBI BookshelfDocument4 pagesCor Pulmonale - StatPearls - NCBI BookshelfAldi RafaelNo ratings yet
- PAH Ann Intern Med 2013Document15 pagesPAH Ann Intern Med 2013waterprincess100% (1)
- Cardiovascular System: by DR - Nuha Abdel GhaffarDocument41 pagesCardiovascular System: by DR - Nuha Abdel GhaffarMohammed Alaa EldeanNo ratings yet
- Manage and Diagnose Acute and Chronic Cor PulmonaleDocument42 pagesManage and Diagnose Acute and Chronic Cor PulmonaleNym Angga SantosaNo ratings yet
- Pulmonic Valve DiseaseDocument22 pagesPulmonic Valve Diseasesarguss14No ratings yet
- Krisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranDocument85 pagesKrisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranSeptian WidiantoNo ratings yet
- Renal Stone Types, Causes and SymptomsDocument29 pagesRenal Stone Types, Causes and Symptomsarim100% (1)
- The Nigrostriatal PathwayDocument13 pagesThe Nigrostriatal Pathwayapi-534201968No ratings yet
- Copar (Nursing)Document9 pagesCopar (Nursing)MariaNo ratings yet
- Focused Ultrasonography For Septic Shock ResuscitationDocument7 pagesFocused Ultrasonography For Septic Shock ResuscitationntnquynhproNo ratings yet
- AAO - External Disease and CorneaDocument19 pagesAAO - External Disease and CorneaJohn Paul VillaflorNo ratings yet
- OBGYN Revalida Review 2019Document74 pagesOBGYN Revalida Review 2019anonymous100% (1)
- Oral CandidiasisDocument4 pagesOral CandidiasisAnish RajNo ratings yet
- Mule AaDocument37 pagesMule AaShabaka KashataNo ratings yet
- Neurologic ExaminationDocument67 pagesNeurologic Examinationሀይደር ዶ.ር100% (1)
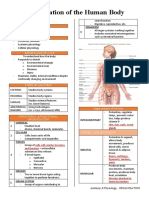
- Organization of the Human BodyDocument8 pagesOrganization of the Human BodyAly HannahNo ratings yet
- Head Injuries ( Lesiones de Cabeza)Document5 pagesHead Injuries ( Lesiones de Cabeza)Camila BenitezNo ratings yet
- Deworming of PetsDocument5 pagesDeworming of PetsRehan Ashraf BandeshaNo ratings yet
- 10th Biology Solved MCQS (Bismillah) EditDocument19 pages10th Biology Solved MCQS (Bismillah) EditSohail Afzal100% (1)
- ACEs FlyerDocument2 pagesACEs Flyermahima sajanNo ratings yet
- Matrix On Somatic Disorders: Luzenne Sanchez Jones PSYC 118X Clinical Psyc TTH 4:30-6:00 March 12, 2020Document5 pagesMatrix On Somatic Disorders: Luzenne Sanchez Jones PSYC 118X Clinical Psyc TTH 4:30-6:00 March 12, 2020Monina JonesNo ratings yet
- A Clinical Decision Support Framework For Heterogeneous Data SourcesDocument10 pagesA Clinical Decision Support Framework For Heterogeneous Data SourcesdineshshaNo ratings yet
- Medical Student Syndrome Bjmp-2019-12-1-A003: British Journal of Medical Practitioners January 2019Document6 pagesMedical Student Syndrome Bjmp-2019-12-1-A003: British Journal of Medical Practitioners January 2019Nabila AjmaliaNo ratings yet
- Tendon Injuries of Hand: DR Saumya AgarwalDocument101 pagesTendon Injuries of Hand: DR Saumya AgarwaltesfahuntekletilahunNo ratings yet
- Corn Pest Surveillance Pre-Inception MeetingDocument41 pagesCorn Pest Surveillance Pre-Inception MeetingMarcJunardJoverNo ratings yet
- DENGUE VIRUS STRAINS AND VECTORSDocument2 pagesDENGUE VIRUS STRAINS AND VECTORSImee Claire PacisNo ratings yet
- Assessment of Tympanic Membrane Perforation in AdultDocument4 pagesAssessment of Tympanic Membrane Perforation in AdultVikrant Vaze100% (1)
- Ayurveda, YogaDocument34 pagesAyurveda, Yogayandi permanaNo ratings yet
- Review of Studies On Flight Attendant Health and Comfort in Airliner CabinsDocument9 pagesReview of Studies On Flight Attendant Health and Comfort in Airliner CabinsStudentNo ratings yet
- J American Geriatrics Society - 2023 - American Geriatrics Society 2023 Updated AGS Beers Criteria For PotentiallyDocument30 pagesJ American Geriatrics Society - 2023 - American Geriatrics Society 2023 Updated AGS Beers Criteria For PotentiallyMikeNo ratings yet
- DIAA0039-StigmaReport 17sp 20210711 PDFDocument28 pagesDIAA0039-StigmaReport 17sp 20210711 PDFIndranil PoddarNo ratings yet
- Tiket Juragan GombalDocument3 pagesTiket Juragan Gombaldhebys suryaniNo ratings yet
- How Do We Walk?: Sujay Galen PT PHD FheaDocument52 pagesHow Do We Walk?: Sujay Galen PT PHD FheaColleen JohnsonNo ratings yet
- ASM 345 Study Guide For Quiz 5 Module 5 - 2014-1Document2 pagesASM 345 Study Guide For Quiz 5 Module 5 - 2014-1Martín CastilloNo ratings yet