You might also like
- Bioethics LectureDocument40 pagesBioethics LecturejeshemaNo ratings yet
- Chronic Non-communicable Diseases in Ghana: Multidisciplinary PerspectivesFrom EverandChronic Non-communicable Diseases in Ghana: Multidisciplinary PerspectivesNo ratings yet
- Notes on Nursing - What It Is, and What It Is Not: With a Chapter From 'Beneath the Banner, Being Narratives of Noble Lives and Brave Deeds' by F. J. CrossFrom EverandNotes on Nursing - What It Is, and What It Is Not: With a Chapter From 'Beneath the Banner, Being Narratives of Noble Lives and Brave Deeds' by F. J. CrossNo ratings yet
- 03 Dilemma & 04 Biomedical Ethics Discorse (Prof Hakimi)Document54 pages03 Dilemma & 04 Biomedical Ethics Discorse (Prof Hakimi)Zuzu FinusNo ratings yet
- The Battle Against Covid-19 Filipino American Healthcare Workers on the Frontlines of the Pandemic ResponseFrom EverandThe Battle Against Covid-19 Filipino American Healthcare Workers on the Frontlines of the Pandemic ResponseNo ratings yet
- Nurses and Their Patients: Informing practice through psychodynamic insightsFrom EverandNurses and Their Patients: Informing practice through psychodynamic insightsNo ratings yet
- Stories of Dignity within Healthcare: Research, narratives and theoriesFrom EverandStories of Dignity within Healthcare: Research, narratives and theoriesNo ratings yet
- Values in NursingDocument1 pageValues in NursingLynette Olavides CalagoNo ratings yet
- Nursing ResearchDocument52 pagesNursing Researchamyrrhielle86% (7)
- Bioethics: Walbert F. Delos Santos, RN - MNDocument43 pagesBioethics: Walbert F. Delos Santos, RN - MNmaidymae lopezNo ratings yet
- Bioethical Issues in End of LifeDocument31 pagesBioethical Issues in End of Lifebotet_2306No ratings yet
- Medical EthicsDocument75 pagesMedical EthicsNenyAriyana100% (2)
- Health Care Ethics: BioethicsDocument9 pagesHealth Care Ethics: BioethicsR-Chian Jose GermanpNo ratings yet
- Ethical Dilemmas in NursingDocument21 pagesEthical Dilemmas in NursingHusain Tamimie100% (2)
- Dorothea Orem'S Self-Care Deficit Nursing Theory: By: Tracy Clarke & Jeanine GrossmanDocument37 pagesDorothea Orem'S Self-Care Deficit Nursing Theory: By: Tracy Clarke & Jeanine Grossmannapper67100% (2)
- Medical EthicsDocument13 pagesMedical EthicsLizbeth Aura CebrianNo ratings yet
- Evidence-Based Nursing Practice ModelsDocument42 pagesEvidence-Based Nursing Practice ModelsVivin Karlina100% (1)
- New insights for defining and diagnosing postpartum hemorrhageDocument7 pagesNew insights for defining and diagnosing postpartum hemorrhageRabbi'ahNo ratings yet
- Human To Human Relationship ModelDocument4 pagesHuman To Human Relationship Modelrj carpsonNo ratings yet
- CNO-Compendium: Understanding Ethical FrameworksDocument42 pagesCNO-Compendium: Understanding Ethical FrameworksdanushaNo ratings yet
- Ethical Problems in Nursing ManagementDocument4 pagesEthical Problems in Nursing ManagementJen Rhae LimNo ratings yet
- Abortion From An Ethical Point of ViewDocument3 pagesAbortion From An Ethical Point of ViewJ David Harvel100% (1)
- Ethical Decision MakingDocument5 pagesEthical Decision Makingapi-491453387No ratings yet
- Nursing TheoryDocument12 pagesNursing TheorydrsabuegNo ratings yet
- AppendicitisDocument8 pagesAppendicitisPhoebe Corazon Cercado100% (1)
- Legal and Ethical Issues PrintDocument8 pagesLegal and Ethical Issues Printbharti deshlahraNo ratings yet
- Ethical Dimension of Nursing Practice WordDocument6 pagesEthical Dimension of Nursing Practice Wordpink096No ratings yet
- Ethic in NursingDocument246 pagesEthic in Nursingsyikir100% (1)
- Legal Aspects of NursingDocument26 pagesLegal Aspects of NursingJasmin Jacob100% (1)
- Ethical Dilemmas in Nursing PDFDocument5 pagesEthical Dilemmas in Nursing PDFtitiNo ratings yet
- Methods of EpidemiologyDocument28 pagesMethods of EpidemiologyAlice sylviya SamuelNo ratings yet
- Nursing Ethics and Moral IssuesDocument22 pagesNursing Ethics and Moral IssuesEnaira Devera Ramos100% (1)
- Legal Aspects of NursingDocument71 pagesLegal Aspects of NursingErl D. Melitante100% (1)
- Ethical Issues in NursingDocument30 pagesEthical Issues in NursingUpendra Yadav100% (2)
- Evolution of nursing and healthcare professionsDocument32 pagesEvolution of nursing and healthcare professionsNatukunda DianahNo ratings yet
- Withholding & Withdrawing Life-Sustaining TreatmentDocument11 pagesWithholding & Withdrawing Life-Sustaining TreatmentDr. Liza Manalo100% (1)
- Belmont Report principles of respect, beneficence and justiceDocument19 pagesBelmont Report principles of respect, beneficence and justiceAmar JitjNo ratings yet
- Introduction To Perioperative NursingDocument19 pagesIntroduction To Perioperative NursingaidaelgamilNo ratings yet
- Jean WatsonDocument14 pagesJean WatsonAndyNo ratings yet
- Charting: Prepared By: Amelia Filio Nacario R.N. MANDocument38 pagesCharting: Prepared By: Amelia Filio Nacario R.N. MANArlyn MendenillaNo ratings yet
- Critical Health Concerns of The 21st CenturyDocument2 pagesCritical Health Concerns of The 21st CenturySafa AamirNo ratings yet
- Unit 8 PPT Psychiatry Lecture NotesDocument24 pagesUnit 8 PPT Psychiatry Lecture NotesDENNIS N. MUÑOZNo ratings yet
- Dorothea Orems Theory of Self Care DeficitDocument35 pagesDorothea Orems Theory of Self Care DeficitDiah Permata SariNo ratings yet
- Evidence-Based Practice: The 5 Steps Nurses Need to Provide Quality CareDocument43 pagesEvidence-Based Practice: The 5 Steps Nurses Need to Provide Quality CareApRil Anne Balanon100% (1)
- Ethical Issues in Pediatric AnesDocument16 pagesEthical Issues in Pediatric AnesrejNo ratings yet
- Human Becoming TheoryDocument3 pagesHuman Becoming Theoryflo_lamontagne100% (1)
- Health Care Ethics 2024Document13 pagesHealth Care Ethics 2024celestineNo ratings yet
- Evidenced Based PracticesDocument12 pagesEvidenced Based PracticesCHRISTINE JOY. MOLINANo ratings yet
- Imogene M. King Conceptual System and Middle Range Theory of Goal AttainmentDocument4 pagesImogene M. King Conceptual System and Middle Range Theory of Goal AttainmentbrylleNo ratings yet
- Maternal Health ServicesDocument24 pagesMaternal Health ServicesMuna Hassan MustafaNo ratings yet
- NCM 108 Module 2021Document117 pagesNCM 108 Module 2021Maia Saivi Omega100% (5)
- Id DocumentDocument2 pagesId Documentali abdel hadiNo ratings yet
- Intro To Solar Energy System FundamentalsDocument26 pagesIntro To Solar Energy System Fundamentalsfabio1199No ratings yet
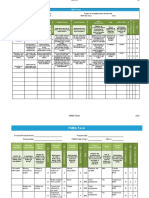
- Fmea Report Test ResultDocument13 pagesFmea Report Test Resultali abdel hadiNo ratings yet
- CD-DVD SleeveDocument1 pageCD-DVD Sleeveali abdel hadiNo ratings yet
- DC Motor - PPTDocument41 pagesDC Motor - PPTali abdel hadiNo ratings yet
- دعوة وقفة تضامنية 29-3-2022 - اعلاميينDocument1 pageدعوة وقفة تضامنية 29-3-2022 - اعلاميينali abdel hadiNo ratings yet
- Reducing Anti-Microbial Resistance of Treatable Sexually-Transmitted Infections in Antenatal CareDocument101 pagesReducing Anti-Microbial Resistance of Treatable Sexually-Transmitted Infections in Antenatal Careali abdel hadiNo ratings yet
- How To Make Doctors LeadersDocument11 pagesHow To Make Doctors Leadersali abdel hadiNo ratings yet
- Case Study: Chapter1:HealthcarequalityandthepatientDocument5 pagesCase Study: Chapter1:Healthcarequalityandthepatientali abdel hadiNo ratings yet
- Healthcare Facilities Management: Lecture 1-Dr - Mohamad Nassereddine HMTM512Document52 pagesHealthcare Facilities Management: Lecture 1-Dr - Mohamad Nassereddine HMTM512ali abdel hadiNo ratings yet
- PRICE LIST 2019-2020: International ProgramsDocument1 pagePRICE LIST 2019-2020: International Programsali abdel hadiNo ratings yet
- Yashal's Ielts Mock 26.21 Ac WritingDocument5 pagesYashal's Ielts Mock 26.21 Ac Writingali abdel hadiNo ratings yet
- Patient Satisfaction and Quality of Nursing CareDocument12 pagesPatient Satisfaction and Quality of Nursing Careali abdel hadiNo ratings yet
- Sweden HealthcareDocument1 pageSweden Healthcareali abdel hadiNo ratings yet
- RepeatFeeCalculator2019 2020Document3 pagesRepeatFeeCalculator2019 2020ali abdel hadiNo ratings yet
- Azcommonproper - WgmaDocument4 pagesAzcommonproper - WgmaLorinelle Castro100% (1)
- Periodic Operational PlanDocument4 pagesPeriodic Operational Planali abdel hadiNo ratings yet
- Information On Student FinancesDocument5 pagesInformation On Student Financesali abdel hadiNo ratings yet
- 32 Ielts Essay Samples Band 9Document34 pages32 Ielts Essay Samples Band 9mh73% (26)
- Undergraduate Programmes Leading To A Primary Degree / Diploma. Fees 2019 - 20Document3 pagesUndergraduate Programmes Leading To A Primary Degree / Diploma. Fees 2019 - 20ali abdel hadiNo ratings yet
- FIBA Asia Cup 2017 - Day 1 TicketDocument2 pagesFIBA Asia Cup 2017 - Day 1 Ticketali abdel hadiNo ratings yet
- Band 7.5 Evaluated Essay 2407 PDFDocument4 pagesBand 7.5 Evaluated Essay 2407 PDFAli HossainNo ratings yet
- List of Synonyms and Antonyms PDFDocument5 pagesList of Synonyms and Antonyms PDFPraveen KumarNo ratings yet
- Parts of Speech, Vocabulary - AnimalsDocument1 pageParts of Speech, Vocabulary - Animalsali abdel hadiNo ratings yet
- Session 6 StrategyDocument40 pagesSession 6 Strategyali abdel hadiNo ratings yet
- Antonyms PDFDocument12 pagesAntonyms PDFRabi ChaudhryNo ratings yet
- Solved Idioms From 1971 To 2015 - Updated PDFDocument58 pagesSolved Idioms From 1971 To 2015 - Updated PDFImranRazaBozdarNo ratings yet
- Session 5 PlanningDocument40 pagesSession 5 Planningali abdel hadiNo ratings yet
- Case Study: Chapter1:HealthcarequalityandthepatientDocument5 pagesCase Study: Chapter1:Healthcarequalityandthepatientali abdel hadiNo ratings yet
- LU-Masters-Healthcare and Quality Management Healthcare Management HCQM411 Healthcare Management HCQM411 2020-2021 Course OutlineDocument22 pagesLU-Masters-Healthcare and Quality Management Healthcare Management HCQM411 Healthcare Management HCQM411 2020-2021 Course Outlineali abdel hadiNo ratings yet
- Marrin - Intelligence Analysis-Turning A Craft Into A ProfessionDocument5 pagesMarrin - Intelligence Analysis-Turning A Craft Into A ProfessionStephen MarrinNo ratings yet
- List of NgosDocument41 pagesList of Ngosdododod23100% (1)
- Motivational Interviewing A Guide For Medical Trainees 1st EditionDocument281 pagesMotivational Interviewing A Guide For Medical Trainees 1st EditionJames89% (9)
- Professional ResumeDocument3 pagesProfessional ResumeUc OhiriNo ratings yet
- M.Sc. Nursing Advance Nursing Practice Unit I-Nursing As A ProfessionDocument66 pagesM.Sc. Nursing Advance Nursing Practice Unit I-Nursing As A ProfessionValarmathiNo ratings yet
- Acute Medicine (Medical Masterclass)Document163 pagesAcute Medicine (Medical Masterclass)Chris Jardine Li100% (1)
- Hospital Tefl VocabularyDocument3 pagesHospital Tefl VocabularymanbgNo ratings yet
- SLMC - Regulating Sri Lanka's Medical ProfessionDocument27 pagesSLMC - Regulating Sri Lanka's Medical ProfessionTrishenth FonsekaNo ratings yet
- Maternal ThesisDocument10 pagesMaternal ThesisMerwynmae PobletinNo ratings yet
- Patient-Centered Communication Review Summarizes Importance of Communication SkillsDocument9 pagesPatient-Centered Communication Review Summarizes Importance of Communication SkillsFernanda BordignonNo ratings yet
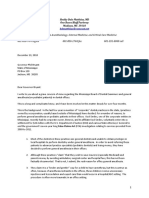
- Matthias Letter To GovernorDocument9 pagesMatthias Letter To GovernorLuke RNo ratings yet
- Editing Chapter1234Document62 pagesEditing Chapter1234pia espanilloNo ratings yet
- Lupton CONSUMERISM, REFLEXIVITY AND THE MEDICAL ENCOUNTERDocument9 pagesLupton CONSUMERISM, REFLEXIVITY AND THE MEDICAL ENCOUNTERdobberer4379No ratings yet
- ELECTROPATHYDocument51 pagesELECTROPATHYBalaji Rao N89% (28)
- ICA GuidlinesDocument465 pagesICA GuidlinesdrtimadamsNo ratings yet
- Stress, Anxiety and Insomnia by Michael MurrayDocument154 pagesStress, Anxiety and Insomnia by Michael MurrayClaireFitzpatrick100% (1)
- Pre Service Training ImpDocument40 pagesPre Service Training ImpAbdulAhadNo ratings yet
- Bridge To Residency Updated 02 08Document21 pagesBridge To Residency Updated 02 08Lucano GómezNo ratings yet
- Dafpus 4Document4 pagesDafpus 4wahyu purnamaNo ratings yet
- Policy Wordings - IOB Health Care Plus Revision PDFDocument30 pagesPolicy Wordings - IOB Health Care Plus Revision PDFgrr.homeNo ratings yet
- HSE - Health Surveillance at WorkDocument27 pagesHSE - Health Surveillance at WorkfullfrenzyNo ratings yet
- JCU Medicine Application FormDocument13 pagesJCU Medicine Application FormmNo ratings yet
- Prinsip Kedokteran Keluarga 2018Document57 pagesPrinsip Kedokteran Keluarga 2018Silvia HandikaNo ratings yet
- PCDC 2009 Spring Gala Tribute BookDocument86 pagesPCDC 2009 Spring Gala Tribute Bookpcdc1993No ratings yet
- Clinical Manual of Psychosomatic Medicine A Guide To ConsultatiDocument565 pagesClinical Manual of Psychosomatic Medicine A Guide To ConsultatiDalal HazelNo ratings yet
- A Textbook of Postpartum HemorrhageDocument496 pagesA Textbook of Postpartum Hemorrhagevalitim89% (9)
- 10 - Jessica Fanny Manobe Assignment 1 Introducing Healthcare Professionals-1Document13 pages10 - Jessica Fanny Manobe Assignment 1 Introducing Healthcare Professionals-1177 Gede Agus Purna YogaNo ratings yet
- From A Pathologist's DeskDocument33 pagesFrom A Pathologist's DeskDr Suvarna NalapatNo ratings yet
- St. Luke's Echocardiogram Patient GuideDocument2 pagesSt. Luke's Echocardiogram Patient Guideteju13aNo ratings yet
- Pay and Conditions Circular MD 4 2023 Final - 0Document31 pagesPay and Conditions Circular MD 4 2023 Final - 0asi basseyNo ratings yet