You might also like
- Table of Leukemias and LymphomasDocument7 pagesTable of Leukemias and LymphomasRhenjay Ferrer Lagoy100% (1)
- 18 Characteristics of Leukemias Lymphomas and MyelomasDocument9 pages18 Characteristics of Leukemias Lymphomas and MyelomasDaphne HernaezNo ratings yet
- Anatomy of Larynx Lecture 7Document21 pagesAnatomy of Larynx Lecture 7sallykamareddine100% (1)
- Mediastinum and Its ContentsDocument11 pagesMediastinum and Its ContentsPap YeeNo ratings yet
- Hemodynamics: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeDocument31 pagesHemodynamics: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeÑäd ÉèmNo ratings yet
- Cardiovascular SystemDocument58 pagesCardiovascular Systemsultan khabeebNo ratings yet
- ANPH-M2-CU8. The HeartDocument20 pagesANPH-M2-CU8. The HeartMary Grace MapulaNo ratings yet
- 2 Medicine HematologyDocument78 pages2 Medicine HematologyAmitNo ratings yet
- AP Chapter 16BDocument35 pagesAP Chapter 16BJay Patel100% (1)
- Hemopoiesis PDFDocument14 pagesHemopoiesis PDFrysnawahyu13No ratings yet
- S0850alug 1670953860959-SEU HDocument56 pagesS0850alug 1670953860959-SEU HAziz KhwajaNo ratings yet
- Anemia BMLTDocument134 pagesAnemia BMLTRajkishor YadavNo ratings yet
- Haemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)Document20 pagesHaemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)shravaniNo ratings yet
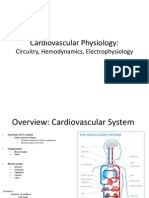
- Cardiovascular Physiology:: Circuitry, Hemodynamics, ElectrophysiologyDocument27 pagesCardiovascular Physiology:: Circuitry, Hemodynamics, Electrophysiologyrsmoney3No ratings yet
- LeukemiaDocument1 pageLeukemiaGomathiRachakondaNo ratings yet
- Physio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionDocument5 pagesPhysio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionAnny AlvrzNo ratings yet
- Anemia-Dr Moses KazevuDocument86 pagesAnemia-Dr Moses KazevuMoses Jr KazevuNo ratings yet
- Microcytic Anemia Causes, Symptoms, and TreatmentDocument33 pagesMicrocytic Anemia Causes, Symptoms, and TreatmentrohitNo ratings yet
- Introduction To Cell PhysiologyDocument149 pagesIntroduction To Cell PhysiologyAlysaNo ratings yet
- Patho Physiology Lecture13Document10 pagesPatho Physiology Lecture13Manar AlzobiNo ratings yet
- Physiology of The Cardiovascular System-CVSDocument56 pagesPhysiology of The Cardiovascular System-CVSAmanuel MaruNo ratings yet
- LSM3212 - Lecture 2-4 BloodDocument59 pagesLSM3212 - Lecture 2-4 BloodAbraham KangNo ratings yet
- Cardiovascular Physiology 4 - Gomez MD PDFDocument65 pagesCardiovascular Physiology 4 - Gomez MD PDFMelissa SalayogNo ratings yet
- Hema Primary DisordersDocument13 pagesHema Primary DisordersMiki NishiharaNo ratings yet
- RBC Physiology and Blood TypingDocument3 pagesRBC Physiology and Blood TypingGabrielle SerranoNo ratings yet
- Pathology of blood and lymphatic vessels overviewDocument55 pagesPathology of blood and lymphatic vessels overviewMhinory OctNo ratings yet
- Composition and Function of Blood ComponentsDocument17 pagesComposition and Function of Blood ComponentsPrakash Kumar Nayak100% (1)
- Skeletal Muscle Contraction MechanismDocument10 pagesSkeletal Muscle Contraction MechanismLiljana StojkovicNo ratings yet
- Plasma Physiology (1-2020) by DR Khaled A AbulfadleDocument9 pagesPlasma Physiology (1-2020) by DR Khaled A AbulfadleUzama Binu AliNo ratings yet
- Lecture 3. Bleeding Disorders Part 1Document31 pagesLecture 3. Bleeding Disorders Part 1Kekelwa Mutumwenu Snr100% (1)
- Chapter 15 - Cardiovascular SystemDocument89 pagesChapter 15 - Cardiovascular SystemOliver Namyalo100% (1)
- Blood, Coagulation of Blood & Bleeding Disorders 12 - 7 - 19Document62 pagesBlood, Coagulation of Blood & Bleeding Disorders 12 - 7 - 19AntarleenaNo ratings yet
- Macrocytic AnemiasDocument28 pagesMacrocytic AnemiasDeepankar SrigyanNo ratings yet
- Oncology Revision Environmental Factors ScreeningDocument299 pagesOncology Revision Environmental Factors ScreeningMourian AmanNo ratings yet
- Haematology-Summary My NotesDocument24 pagesHaematology-Summary My NotesToria053No ratings yet
- Lecture 6 Cardiovascular: Vascular System - The HemodynamicsDocument70 pagesLecture 6 Cardiovascular: Vascular System - The HemodynamicsAndreea ŞtefănescuNo ratings yet
- Red Cell MorphologyDocument5 pagesRed Cell MorphologyClaire NicoleNo ratings yet
- Blood ComponentsDocument17 pagesBlood ComponentsJohnSmithNo ratings yet
- Blood Components Where Do They Come From?: Introduction To HaematologyDocument11 pagesBlood Components Where Do They Come From?: Introduction To Haematologydorsa koraeiNo ratings yet
- Chapter 11: Blood 11.1 Functions of Blood: - 91% Water - 7% Proteins (Dissolved)Document3 pagesChapter 11: Blood 11.1 Functions of Blood: - 91% Water - 7% Proteins (Dissolved)Jennifer HerediaNo ratings yet
- Haemoglobin: Higher The Partial Pressure, The Higher The AffinityDocument2 pagesHaemoglobin: Higher The Partial Pressure, The Higher The Affinitydebbie96No ratings yet
- A&P 302 - Respiratory NotesDocument31 pagesA&P 302 - Respiratory NotesBethanyNo ratings yet
- Anemia Its Laboratory DiagnosisDocument146 pagesAnemia Its Laboratory DiagnosisCh M MushahidNo ratings yet
- HIS.K.1.Histology of BloodDocument16 pagesHIS.K.1.Histology of BloodMayaPasaribuNo ratings yet
- PLEURAL EFFUSION CAUSES AND DIAGNOSISDocument52 pagesPLEURAL EFFUSION CAUSES AND DIAGNOSISvaishnaviNo ratings yet
- THROMBOSISDocument18 pagesTHROMBOSISShruti Verma100% (1)
- Control of Blood Tissue Blood Flow: Faisal I. Mohammed, MD, PHDDocument25 pagesControl of Blood Tissue Blood Flow: Faisal I. Mohammed, MD, PHDManohar SinghNo ratings yet
- Blood 12-6-2018Document42 pagesBlood 12-6-2018Noor Fatima100% (1)
- Welcome To Seminar: Dr. Aysha Sabiha Dr. Maimuna Sayeed Dr. Sharmin Akter Luna Residents (Phase-A)Document124 pagesWelcome To Seminar: Dr. Aysha Sabiha Dr. Maimuna Sayeed Dr. Sharmin Akter Luna Residents (Phase-A)interna MANADONo ratings yet
- CBC Reviewer Anaphy LabDocument9 pagesCBC Reviewer Anaphy LabARVINE JUSTINE CORPUZNo ratings yet
- 4 Apr - Bleeding DisordersDocument50 pages4 Apr - Bleeding DisordersAhmed SarfarazNo ratings yet
- CHR InflammationDocument33 pagesCHR InflammationAlnzeer6No ratings yet
- RBC Formation, Anemia, WBC FunctionDocument28 pagesRBC Formation, Anemia, WBC FunctionlifecostNo ratings yet
- Progenitor Heart Cells Lie in The Epiblast, Immediately Adjacent To TheDocument15 pagesProgenitor Heart Cells Lie in The Epiblast, Immediately Adjacent To TheJehangir AllamNo ratings yet
- Haematology MCQ ExamDocument18 pagesHaematology MCQ Examaminata6No ratings yet
- Bleeding Disorders: LCDR Art GeorgeDocument54 pagesBleeding Disorders: LCDR Art Georgesatya_mdsNo ratings yet
- The Cardiac Cycle: Chapter 19Document62 pagesThe Cardiac Cycle: Chapter 19BishwambherNo ratings yet
- HematologyDocument34 pagesHematologyAnne Angue GonzalesNo ratings yet
- Malignant Lymphomas: DR Nilukshi PereraDocument48 pagesMalignant Lymphomas: DR Nilukshi PereraThaveeshaLindsayWhiteNo ratings yet
- Malignant Lymphomas: DR Nilukshi PereraDocument48 pagesMalignant Lymphomas: DR Nilukshi PereraThaveeshaLindsayWhiteNo ratings yet
- Understanding PancytopeniaDocument68 pagesUnderstanding PancytopeniaThaveeshaLindsayWhiteNo ratings yet
- 3-T and Sicke Cell Disease 2016Document68 pages3-T and Sicke Cell Disease 2016ThaveeshaLindsayWhiteNo ratings yet
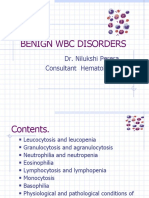
- Benign WBC Disorders: Dr. Nilukshi Perera Consultant HematologistDocument31 pagesBenign WBC Disorders: Dr. Nilukshi Perera Consultant HematologistThaveeshaLindsayWhiteNo ratings yet
- Megaloblastic and Other Macrocytic Anaemia: Dr. Nilukshi Perera Consultant HaematologistDocument58 pagesMegaloblastic and Other Macrocytic Anaemia: Dr. Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNo ratings yet
- Megaloblastic and Other Macrocytic Anaemia: Dr. Nilukshi Perera Consultant HaematologistDocument58 pagesMegaloblastic and Other Macrocytic Anaemia: Dr. Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNo ratings yet
- Patient Safety GuideDocument272 pagesPatient Safety Guidejuanlaplaya100% (1)
- English Specimen Paper 1 2018Document8 pagesEnglish Specimen Paper 1 2018ThaveeshaLindsayWhiteNo ratings yet
- Dr. Nilukshi Perera Consultant HaematologistDocument128 pagesDr. Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNo ratings yet
- 1113 Lower Secondary Science Curriculum Framework 2018 - v2 - tcm143-498591Document16 pages1113 Lower Secondary Science Curriculum Framework 2018 - v2 - tcm143-498591elena100% (2)
- Ethics and Cloning: Invited ReviewDocument7 pagesEthics and Cloning: Invited ReviewHammadNo ratings yet
- Tumor Markers in Clinical Practice: General Principles and GuidelinesDocument8 pagesTumor Markers in Clinical Practice: General Principles and GuidelinesNurmalia SariNo ratings yet
- 858 3068 1 PBDocument7 pages858 3068 1 PBMelody DacanayNo ratings yet
- Histophysiology+of+the+Skin+for+Vula+ Dr+MowlaDocument28 pagesHistophysiology+of+the+Skin+for+Vula+ Dr+MowlaYaaseen GallantNo ratings yet
- 10th Science QN Sep-20Document11 pages10th Science QN Sep-20santhoshsanthosh20202021No ratings yet
- DVD Worksheet Unit 5Document4 pagesDVD Worksheet Unit 5Victor RoblesNo ratings yet
- Name - Date - Period - Mutations WorksheetDocument4 pagesName - Date - Period - Mutations WorksheetEric CalderónNo ratings yet
- Anatomy and Physiology Day 2Document32 pagesAnatomy and Physiology Day 2Lake JazzNo ratings yet
- BT20204 (Cell Biology) Lecture 1 - Cell Theory and Origin of CellsDocument15 pagesBT20204 (Cell Biology) Lecture 1 - Cell Theory and Origin of Cellstagore TNo ratings yet
- Protein Synthesis WorksheetDocument2 pagesProtein Synthesis WorksheetEderlyn Zate100% (1)
- Types of Betta Fish - All Tail, Color, & Pattern VariationsDocument34 pagesTypes of Betta Fish - All Tail, Color, & Pattern VariationsCrunch 69No ratings yet
- Applications of Nanotechnology in Tissue EngineeringDocument22 pagesApplications of Nanotechnology in Tissue EngineeringYuval SteimbergNo ratings yet
- Animal ModelsDocument22 pagesAnimal ModelsM.anwar KhanNo ratings yet
- Gen Micro Micro D&R AgamDocument157 pagesGen Micro Micro D&R AgamNirosha Arul100% (1)
- Subject: Science Quarter: First Quarter Grade Level: 9 TopicsDocument9 pagesSubject: Science Quarter: First Quarter Grade Level: 9 TopicsMary Grace Corpuz100% (1)
- Idler Et Al. (2014) - Idler, C., Venus, J., & Kamm, B. (2014) - Microorganisms For The Production of Lactic Acid and Organic LactatesDocument49 pagesIdler Et Al. (2014) - Idler, C., Venus, J., & Kamm, B. (2014) - Microorganisms For The Production of Lactic Acid and Organic LactatesCaitlyn Danielle Ogay SeeNo ratings yet
- Muscle Contraction WorksheetDocument4 pagesMuscle Contraction WorksheetCharles VollmersNo ratings yet
- Protein Synthesis - WorksheetDocument7 pagesProtein Synthesis - WorksheetMaisha IslamNo ratings yet
- Chapter 13Document56 pagesChapter 13Hậu VũNo ratings yet
- Dentin and Pulp ComplexDocument130 pagesDentin and Pulp ComplexAurthi ElamparithiNo ratings yet
- EssentialDocument34 pagesEssentialAdolfo López100% (1)
- Fundamentals of ReproductionDocument24 pagesFundamentals of ReproductionMengstu NegashNo ratings yet
- Full Download Biochemistry A Short Course 2nd Edition Tymoczko Test BankDocument6 pagesFull Download Biochemistry A Short Course 2nd Edition Tymoczko Test Bankgelnernita23741372100% (33)
- SIYENSIKULADocument3 pagesSIYENSIKULANoob KidNo ratings yet
- Introduction To Marine Biology 4th Edition Karleskint Turner Small Test BankDocument18 pagesIntroduction To Marine Biology 4th Edition Karleskint Turner Small Test Bankteresastoneniegwrjcyt100% (27)
- Biology ReviewDocument6 pagesBiology Reviewmj espanolaNo ratings yet
- Dermatologica Sinica: Ai-Young LeeDocument7 pagesDermatologica Sinica: Ai-Young LeeNatta ApucaranaNo ratings yet
- Nanomaterials For Environmental and Agricultural Sectors 9789819928743Document278 pagesNanomaterials For Environmental and Agricultural Sectors 9789819928743J MrNo ratings yet
- Phylogenetic Tree - WikipediaDocument12 pagesPhylogenetic Tree - WikipediaxbsdNo ratings yet
- Practice Exam Questions For MusclesDocument2 pagesPractice Exam Questions For MusclesTracy SelkNo ratings yet