You might also like
- Horse Anatomy, A Coloring AtlasDocument185 pagesHorse Anatomy, A Coloring AtlasMartyna MałżNo ratings yet
- Stretching Routine For The SplitsDocument2 pagesStretching Routine For The SplitsmsmellyNo ratings yet
- The Colorado Experiment - Fact or Fiction - T NationDocument18 pagesThe Colorado Experiment - Fact or Fiction - T NationCaio RossiNo ratings yet
- Nirvana Face Reading DocumentDocument4 pagesNirvana Face Reading DocumentLuminita Telecan100% (1)
- LA Third YearDocument221 pagesLA Third Yearعلي الاسديNo ratings yet
- Local Anesthesia in Pediatric Dentistry Lecture Students 2009 MDocument88 pagesLocal Anesthesia in Pediatric Dentistry Lecture Students 2009 MIoana DănilăNo ratings yet
- Local Anesthesia For Dental ChildDocument23 pagesLocal Anesthesia For Dental ChildDr. Abdulsalam Awas Dental CenterNo ratings yet
- Nasopalatine Nerve BlockDocument29 pagesNasopalatine Nerve Blockoutright RohitNo ratings yet
- Simple Technique For Lip and Nasolabial Fold Anesthesia For Injectable FillersDocument3 pagesSimple Technique For Lip and Nasolabial Fold Anesthesia For Injectable FillersGina CastilloNo ratings yet
- Anesthetic Considerations in Dental SpecialtiesDocument10 pagesAnesthetic Considerations in Dental SpecialtiesOmar FawazNo ratings yet
- Local Anesthesia (LA) Techniques in Dentistry and Maxillofacial SurgeryDocument106 pagesLocal Anesthesia (LA) Techniques in Dentistry and Maxillofacial SurgeryTerefe AlemayehuNo ratings yet
- Instruments of L.A Lec.3Document6 pagesInstruments of L.A Lec.3Shahad MohmmedNo ratings yet
- ENGanesthesiamanndibleDocument48 pagesENGanesthesiamanndibleRoxanaAnaHociungNo ratings yet
- Injection Techniques For Regional Anesthesia: Contents of CartridgeDocument27 pagesInjection Techniques For Regional Anesthesia: Contents of CartridgeAisyah Arina NurhafizahNo ratings yet
- Anastesi TopikalDocument10 pagesAnastesi TopikallamhotfarmaNo ratings yet
- Maxillary Anesthetic TechniquesDocument55 pagesMaxillary Anesthetic TechniquesMera Emad100% (4)
- Presentation 1Document46 pagesPresentation 1anamiqbalNo ratings yet
- Screenshot 2021-07-04 at 11.16.20 PMDocument41 pagesScreenshot 2021-07-04 at 11.16.20 PMMariam ElshennawyNo ratings yet
- Local Anesthesia in Peadiatric Dentistry: Presented By: DR - Walija Ansari & Dr. Yousuf Ahmed KhanDocument24 pagesLocal Anesthesia in Peadiatric Dentistry: Presented By: DR - Walija Ansari & Dr. Yousuf Ahmed KhanChaudhry Abdullah DeuNo ratings yet
- Administration of Local Anaesthetic in DentistryDocument6 pagesAdministration of Local Anaesthetic in DentistryridaNo ratings yet
- E O N B T: Extra Oral Nerve Block TechniquesDocument26 pagesE O N B T: Extra Oral Nerve Block Techniquesanhca4519No ratings yet
- Maxillaary AnesthesiaDocument44 pagesMaxillaary AnesthesiaAlex HaileyesusNo ratings yet
- Mandibular Injection TechniquesDocument91 pagesMandibular Injection TechniquesRobins Dhakal100% (3)
- Dntal StentsDocument2 pagesDntal StentsMuhammad UzairNo ratings yet
- Failure of Inferior Alveolar Nerve Block: Exploring The AlternativesDocument4 pagesFailure of Inferior Alveolar Nerve Block: Exploring The Alternativesthinkerbell_adaNo ratings yet
- 10.1007@s00784 017 2248 2Document7 pages10.1007@s00784 017 2248 2IndahSerafikaNo ratings yet
- General Practical Aspects: Local Anesthetic ArmamentariumDocument28 pagesGeneral Practical Aspects: Local Anesthetic Armamentariumayman moaed alyasenNo ratings yet
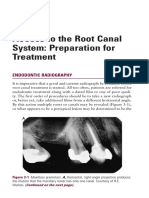
- Access To The Root Canal System: Preparation For Treatment: Endodontic RadiographyDocument13 pagesAccess To The Root Canal System: Preparation For Treatment: Endodontic RadiographyMonika LohakpureNo ratings yet
- Administration of Local Anaesthetic in DentistryDocument5 pagesAdministration of Local Anaesthetic in DentistryridaNo ratings yet
- Maxillary Techniques LecturesDocument151 pagesMaxillary Techniques Lecturespeter samaanNo ratings yet
- Maxillary Techniques LecturesDocument151 pagesMaxillary Techniques Lecturespeter samaanNo ratings yet
- Eksodonsi: Anestesi Lokal & EkstraksiDocument26 pagesEksodonsi: Anestesi Lokal & EkstraksiSusanna Arie KNo ratings yet
- Local Anesthetic TechniquesDocument81 pagesLocal Anesthetic TechniquesMohanad BraziNo ratings yet
- 3-Pain Control in EndodonticsDocument18 pages3-Pain Control in EndodonticsrvmqdpzbjzNo ratings yet
- Jurnal KonsDocument11 pagesJurnal KonsBudhi KaromaNo ratings yet
- Dental and Health Sciences 3: Additional La TechniquesDocument33 pagesDental and Health Sciences 3: Additional La TechniquesAndreea MihaelaNo ratings yet
- Endo Lec 4thDocument123 pagesEndo Lec 4thAli AssimNo ratings yet
- Eksodonsi: Anestesi Lokal & Ekstraksi GigiDocument31 pagesEksodonsi: Anestesi Lokal & Ekstraksi GigiDella AmandaNo ratings yet
- Local Anesthesia - Nerve Blocks & ComplicationsDocument85 pagesLocal Anesthesia - Nerve Blocks & ComplicationsArchanaNo ratings yet
- Local Anesthetics For EndodoDocument25 pagesLocal Anesthetics For EndodowickyliaoNo ratings yet
- IntJOralHealthDent 8-3-256 258Document3 pagesIntJOralHealthDent 8-3-256 258MutiaRamadhantiiNo ratings yet
- Oral Surgical ComplicationsDocument81 pagesOral Surgical ComplicationsMara CiocoNo ratings yet
- Simple Anesthesia TechniqueDocument3 pagesSimple Anesthesia TechniqueBharathiNo ratings yet
- Injection Technique: Kirana Lina G., DRGDocument45 pagesInjection Technique: Kirana Lina G., DRGFinnyalfNo ratings yet
- Local Anaesthesia 3Document8 pagesLocal Anaesthesia 3محمد عماد علي احمدNo ratings yet
- Types and Techniques of Mandibular Nerve Block: Dr. Said Ahmed MohamedDocument33 pagesTypes and Techniques of Mandibular Nerve Block: Dr. Said Ahmed MohamedHudh HudNo ratings yet
- Removal of Obstructions From Root Canal Such As Separated InstrumentsDocument8 pagesRemoval of Obstructions From Root Canal Such As Separated InstrumentsCristinaNo ratings yet
- Anesthesia: Essays and Researches Inferior Alveolar Nerve Block: Alternative TechniqueDocument6 pagesAnesthesia: Essays and Researches Inferior Alveolar Nerve Block: Alternative TechniqueMaqbul AlamNo ratings yet
- Pain ControlDocument88 pagesPain ControlShubham KingraNo ratings yet
- CLOI Kmmereretal.2017 ILAIANBExtractionsDocument8 pagesCLOI Kmmereretal.2017 ILAIANBExtractionsRohma DwiNo ratings yet
- Complication & Failure of ImplantsDocument82 pagesComplication & Failure of ImplantsDrIbrahimShaikhNo ratings yet
- Eksodonsi: Anestesi Lokal & EkstraksiDocument28 pagesEksodonsi: Anestesi Lokal & EkstraksiRicky LeoNo ratings yet
- 2-Fluid Control and Soft TissuDocument6 pages2-Fluid Control and Soft Tissupxb8dhqgs9No ratings yet
- Evaluation of Local Anaesthetic Failures in Dental PracticeDocument6 pagesEvaluation of Local Anaesthetic Failures in Dental PracticenrlNo ratings yet
- Hand Anesthesi A: Roll 60 Yassine NSANZABAGANWADocument22 pagesHand Anesthesi A: Roll 60 Yassine NSANZABAGANWAPineapple100% (1)
- Anaesthesia in Ophthalmology 001Document37 pagesAnaesthesia in Ophthalmology 001pranab2506No ratings yet
- Reed, K, 2012Document11 pagesReed, K, 2012Felipe LarraínNo ratings yet
- E Book BM 1Document7 pagesE Book BM 1najma byvirlianaNo ratings yet
- LA TechDocument46 pagesLA TechLama KhalidNo ratings yet
- ENGanesthesiamaxillaryDocument25 pagesENGanesthesiamaxillaryRoxanaAnaHociungNo ratings yet
- Impression Techniques in Implant Dentistry: Susanna S Brainerd, Dr. Bindu R NayarDocument12 pagesImpression Techniques in Implant Dentistry: Susanna S Brainerd, Dr. Bindu R NayarMaqbul AlamNo ratings yet
- Surgical Instruments: Periodontology DB41ADocument58 pagesSurgical Instruments: Periodontology DB41ANicole LamNo ratings yet
- Chapter 36 - Oral & Amp Maxillofacial Regional AnesthesiaDocument35 pagesChapter 36 - Oral & Amp Maxillofacial Regional AnesthesiaLaura PeñalozaNo ratings yet
- Congestive Heart FailureDocument39 pagesCongestive Heart FailureEthiopia TekdemNo ratings yet
- Physical DiagnosisDocument83 pagesPhysical DiagnosisEthiopia TekdemNo ratings yet
- Valvular Heart DiseasesDocument60 pagesValvular Heart DiseasesEthiopia TekdemNo ratings yet
- Gyni History TalkingDocument61 pagesGyni History TalkingEthiopia TekdemNo ratings yet
- Schizophrenia: DR .TibebuDocument44 pagesSchizophrenia: DR .TibebuEthiopia TekdemNo ratings yet
- Interview in PsychiatryDocument34 pagesInterview in PsychiatryEthiopia TekdemNo ratings yet
- Dr. Temesgen Chali (MD) : Chapter One Introduction To PathologyDocument97 pagesDr. Temesgen Chali (MD) : Chapter One Introduction To PathologyEthiopia TekdemNo ratings yet
- Early Methods of Diagnostic in Oral MedicineDocument26 pagesEarly Methods of Diagnostic in Oral MedicineEthiopia TekdemNo ratings yet
- Pengantar Sistem IntegumenDocument21 pagesPengantar Sistem IntegumenMasniahNo ratings yet
- Physiology vs. Anatomy: by Sarah C.P. Willaims Medically Reviewed by Minesh Khatri, MD On July 28, 2021Document2 pagesPhysiology vs. Anatomy: by Sarah C.P. Willaims Medically Reviewed by Minesh Khatri, MD On July 28, 2021exo oxeNo ratings yet
- Print Version - Five Tibetan RitesDocument12 pagesPrint Version - Five Tibetan RitesJon Fullon Te100% (1)
- The Essential Identity of The Klippel-Feil Syndrome and IniencephalyDocument16 pagesThe Essential Identity of The Klippel-Feil Syndrome and IniencephalyIsolda Alanna RlNo ratings yet
- Soal Unas UGMDocument8 pagesSoal Unas UGMMonik AlamandaNo ratings yet
- Overhead Transparency Human AtlasDocument34 pagesOverhead Transparency Human Atlasdr tamerNo ratings yet
- Radhika Sharma Medical Reports and Prescription (BA LLB Sem 5, 02719103821)Document5 pagesRadhika Sharma Medical Reports and Prescription (BA LLB Sem 5, 02719103821)radhikachitvansharma1No ratings yet
- Principles of Lesion Localization in Neurology - University of MiamiDocument35 pagesPrinciples of Lesion Localization in Neurology - University of MiamiErick AlbanNo ratings yet
- Stretching and Flexibility: How To StretchDocument11 pagesStretching and Flexibility: How To StretchkontakcNo ratings yet
- Chronology of Human Dentition & Tooth Numbering SystemDocument54 pagesChronology of Human Dentition & Tooth Numbering Systemdr parveen bathla100% (4)
- Biomechanics & Joint Replacement of The Knee: PGI Balisi JI Cabalza JI Feliciano JI Fernandez A. JI Fernandez KDocument46 pagesBiomechanics & Joint Replacement of The Knee: PGI Balisi JI Cabalza JI Feliciano JI Fernandez A. JI Fernandez KGio BalisiNo ratings yet
- Biomechanics of Advanced Tennis: January 2003Document7 pagesBiomechanics of Advanced Tennis: January 2003Katrien BalNo ratings yet
- Nerve Compression (Entrapment) SyndromeDocument23 pagesNerve Compression (Entrapment) SyndromeTrending razeNo ratings yet
- HAP Question Bank Sem 2 B PharmDocument4 pagesHAP Question Bank Sem 2 B PharmJeswin AntoNo ratings yet
- Long - Neuropsychology of Emotion PDFDocument8 pagesLong - Neuropsychology of Emotion PDFFlorencia Carla CossiniNo ratings yet
- Obstructive UropathyDocument3 pagesObstructive UropathyGerardLum100% (1)
- Core & Pelvis - The Anterior Oblique SystemDocument4 pagesCore & Pelvis - The Anterior Oblique Systemryan9871No ratings yet
- Chevannese Ellis - Circ Class WorkDocument3 pagesChevannese Ellis - Circ Class WorkChevannese EllisNo ratings yet
- Orientation RelationDocument32 pagesOrientation Relationshameen kumarNo ratings yet
- College of Physical Therapy Sem2Document10 pagesCollege of Physical Therapy Sem2karen magallanesNo ratings yet
- Mri Brain and Orbits: Name Age/Gender Ref. by MRN Report Date C-5-86311 Reg. DateDocument2 pagesMri Brain and Orbits: Name Age/Gender Ref. by MRN Report Date C-5-86311 Reg. DateArslan MunawarNo ratings yet
- Arthur MacNeill Horton Jr. EdD ABPP ABPN, Lawrence C. Hartlage PHD ABPP ABPN - Handbook of Forensic Neuropsychology-Springer Publishing Company (2003) PDFDocument569 pagesArthur MacNeill Horton Jr. EdD ABPP ABPN, Lawrence C. Hartlage PHD ABPP ABPN - Handbook of Forensic Neuropsychology-Springer Publishing Company (2003) PDF'Minerva AlejandraNo ratings yet
- Distasis RectiDocument6 pagesDistasis Rectigkarthispt100% (2)
- The Essential Anatomical Subunit Approximation Unilateral Cleft Lip RepairDocument4 pagesThe Essential Anatomical Subunit Approximation Unilateral Cleft Lip Repairanggita ningratNo ratings yet
- General MyologyDocument26 pagesGeneral MyologyikawaraztutyNo ratings yet
- Basic Anatomy: First YearDocument10 pagesBasic Anatomy: First YearRick DasNo ratings yet