You might also like
- Ocular InjuryDocument46 pagesOcular InjurysnyNo ratings yet
- Ophthalmology EmergenciesDocument60 pagesOphthalmology Emergenciesasraf amirullahNo ratings yet
- Ocular Emergency: Dokter Muda Kevin Chikrista I4061172039Document39 pagesOcular Emergency: Dokter Muda Kevin Chikrista I4061172039kevin chikristaNo ratings yet
- Treat Ocular Emergencies FastDocument29 pagesTreat Ocular Emergencies FastMohammad Farouq Omar100% (3)
- Lecture Injuries of Organ of Vision.Document47 pagesLecture Injuries of Organ of Vision.rajarajachozhan139No ratings yet
- Ocular Trauma Guide - Causes, Symptoms & TreatmentsDocument46 pagesOcular Trauma Guide - Causes, Symptoms & TreatmentssightbdNo ratings yet
- Call ophthalmology immediately. Do not examine further or perform any procedures that could worsen injury. Cover eye securely and stabilizeDocument32 pagesCall ophthalmology immediately. Do not examine further or perform any procedures that could worsen injury. Cover eye securely and stabilizenavenNo ratings yet
- Opthalmic Emergencies PresentationDocument85 pagesOpthalmic Emergencies PresentationvictoreffiomNo ratings yet
- Pediatric Ocular EmergenciesDocument71 pagesPediatric Ocular EmergenciesenzomontresolNo ratings yet
- Trauma To The GlobeDocument19 pagesTrauma To The Globejollyday90No ratings yet
- Trauma and Ocular Emergencies: An OverviewDocument35 pagesTrauma and Ocular Emergencies: An OverviewMochaLover100% (2)
- Ocular Trauma Dr. As-Ali 2 OktoberDocument61 pagesOcular Trauma Dr. As-Ali 2 OktoberYama Piniel FrimantamaNo ratings yet
- Eye Trauma Guide: Incidence, Evaluation, and TreatmentDocument75 pagesEye Trauma Guide: Incidence, Evaluation, and TreatmentAmanuel GirmayeNo ratings yet
- 02 Trauma Oculi - Dr. Tutuk Wibowo Chamidy, SP.MDocument60 pages02 Trauma Oculi - Dr. Tutuk Wibowo Chamidy, SP.MDissa Yulianita SuryaniNo ratings yet
- Anisman Acute Vision LossDocument68 pagesAnisman Acute Vision Lossarnol3090No ratings yet
- Ocular EmergencyDocument86 pagesOcular EmergencyMohammadNo ratings yet
- L9 Cataract and Ocular PharmDocument26 pagesL9 Cataract and Ocular PharmSofíaGriggsNo ratings yet
- Management of Ocular BurnsDocument53 pagesManagement of Ocular BurnsPeter AbikoyeNo ratings yet
- Trauma MataDocument57 pagesTrauma MataFatmala Umi MaisarahNo ratings yet
- Cataract 2 Lecture MBBS by Prof Munim SuriDocument37 pagesCataract 2 Lecture MBBS by Prof Munim SuriMunim SuriNo ratings yet
- Ocular Injuries and EmergenciesDocument60 pagesOcular Injuries and Emergenciesarnol3090100% (1)
- Common Ocular EmergenciesDocument33 pagesCommon Ocular EmergenciesMaimoona AimanNo ratings yet
- Objective - Subjective Eye Examination-Referral System and When To ReferDocument56 pagesObjective - Subjective Eye Examination-Referral System and When To ReferClara Sainuka100% (1)
- Common Eye ConditionsDocument35 pagesCommon Eye ConditionsElukoti BhosleNo ratings yet
- Eye Trauma: Penetrating and BluntDocument68 pagesEye Trauma: Penetrating and BluntSurgicalgownNo ratings yet
- Common Eye Diseases 2022Document33 pagesCommon Eye Diseases 2022Shia LevyNo ratings yet
- Ocular Trauma: H. Amiruddin, DR., Spm. Rsud Arifin Achmad PekanbaruDocument22 pagesOcular Trauma: H. Amiruddin, DR., Spm. Rsud Arifin Achmad PekanbaruNovasiska Indriyani HutajuluNo ratings yet
- OCULAR TRAUMA GUIDEDocument69 pagesOCULAR TRAUMA GUIDERaNo ratings yet
- The Red EyeDocument45 pagesThe Red EyeIsraa AlaaNo ratings yet
- Emergency Eye ConditionsDocument70 pagesEmergency Eye Conditionsalifiah nabillaNo ratings yet
- Everything I Say Will Be On The EXAM !!!Document49 pagesEverything I Say Will Be On The EXAM !!!Tanani 102014007No ratings yet
- Opt Halm OlogyDocument87 pagesOpt Halm OlogyAya MahmoudNo ratings yet
- Ophthalmologic Findings Suggesting Systemic Conditions: Cynthia V. Verzosa, MD, Dpbo, MSCDocument86 pagesOphthalmologic Findings Suggesting Systemic Conditions: Cynthia V. Verzosa, MD, Dpbo, MSCCynthia VerzosaNo ratings yet
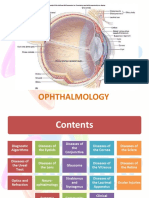
- OphthalmologyDocument144 pagesOphthalmologyrosaririsNo ratings yet
- Ocular EmergenciesDocument26 pagesOcular EmergenciesYukianesa100% (1)
- Common Ocular DisordersDocument108 pagesCommon Ocular DisordersKa SalvinNo ratings yet
- Lecture Chronic Red EyeDocument25 pagesLecture Chronic Red Eyejustforfun219No ratings yet
- Eye Exam Techniques and Ophthalmic Equipment GuideDocument59 pagesEye Exam Techniques and Ophthalmic Equipment Guidehenok birukNo ratings yet
- ENT LESSON 8 (1)Document45 pagesENT LESSON 8 (1)favourednancie9No ratings yet
- Cataract 1 MBBS Lecture by Prof Munim SuriDocument33 pagesCataract 1 MBBS Lecture by Prof Munim SuriMunim SuriNo ratings yet
- Cataract 1 Lecture PmcajkDocument33 pagesCataract 1 Lecture PmcajkAbdul Munim KhanNo ratings yet
- CATARACTDocument12 pagesCATARACTTaiwo IfedolapoNo ratings yet
- Ocular OrbitaDocument11 pagesOcular OrbitaMuhammad Nur SidiqNo ratings yet
- Eye Problems: Dr. Gitalisa Andayani, SPMDocument88 pagesEye Problems: Dr. Gitalisa Andayani, SPMhasanajNo ratings yet
- 03 Eyes and Ears 2 1Document62 pages03 Eyes and Ears 2 1Gerald BatugalNo ratings yet
- Kegawatdarutan Mata Dalam Konsep DogaDocument68 pagesKegawatdarutan Mata Dalam Konsep DogaDavi DzikirianNo ratings yet
- Eye Manifestations of Systemic DiseasesDocument77 pagesEye Manifestations of Systemic DiseasesBamusi ChimwemweNo ratings yet
- K.15 Ophtalmologic EmergenciesDocument35 pagesK.15 Ophtalmologic EmergenciesZikri Putra Lan Lubis100% (1)
- Ocular EmergDocument41 pagesOcular EmergMohd SyazrinNo ratings yet
- Eye Disorders: Beena Davis, RN, MSN N243Document24 pagesEye Disorders: Beena Davis, RN, MSN N243Faiz RangariNo ratings yet
- Hyphema - Traumatic Eye Bleeding Diagnostic and Treatment GuideDocument9 pagesHyphema - Traumatic Eye Bleeding Diagnostic and Treatment GuideMutiara SazkiaNo ratings yet
- External Eye Assessment and ManagementDocument18 pagesExternal Eye Assessment and ManagementGLadys GegareNo ratings yet
- Glaucoma & CataractDocument53 pagesGlaucoma & CataractBenita100% (1)
- OPHTHALMOLOGY COMPANIONDocument31 pagesOPHTHALMOLOGY COMPANIONTaiwo IfedolapoNo ratings yet
- Care and management of clients with eye and ear disordersDocument35 pagesCare and management of clients with eye and ear disordersKristine Joy RevañoNo ratings yet
- Eyelids AdnexalDocument52 pagesEyelids AdnexalRushdaNo ratings yet
- Revision Ophtha 2023Document189 pagesRevision Ophtha 2023Wahib ZaidiNo ratings yet
- Glaucoma: Defitaria Permatasari I11109005Document46 pagesGlaucoma: Defitaria Permatasari I11109005yusufharkianNo ratings yet
- Ocular TraumaDocument44 pagesOcular TraumaKing DonNo ratings yet
- Ocular Trauma FeedbackDocument18 pagesOcular Trauma FeedbackCynthia VerzosaNo ratings yet
- 8 Part Eye ExamDocument32 pages8 Part Eye ExamCynthia VerzosaNo ratings yet
- Systemic Diseases with Ocular Manifestations: An OverviewDocument64 pagesSystemic Diseases with Ocular Manifestations: An OverviewCynthia VerzosaNo ratings yet
- Ocular Trauma and Emergencies New TemplateDocument51 pagesOcular Trauma and Emergencies New TemplateCynthia VerzosaNo ratings yet
- Ophthalmologic Findings Suggesting Systemic Conditions: Cynthia V. Verzosa, MD, Dpbo, MSCDocument86 pagesOphthalmologic Findings Suggesting Systemic Conditions: Cynthia V. Verzosa, MD, Dpbo, MSCCynthia VerzosaNo ratings yet
- Strabismus: Cynthia V. Verzosa, MD, Dpbo, MSCDocument41 pagesStrabismus: Cynthia V. Verzosa, MD, Dpbo, MSCCynthia VerzosaNo ratings yet
- Case Presentation CVV v2 VietnamDocument85 pagesCase Presentation CVV v2 VietnamCynthia VerzosaNo ratings yet
- Mundipharma Lecture Tools, Tips, Tricks CVVDocument61 pagesMundipharma Lecture Tools, Tips, Tricks CVVCynthia VerzosaNo ratings yet
- Minimally Invasive Glaucoma Surgery (Migs) : Cynthia V. Verzosa, MD, Dpbo, MSCDocument50 pagesMinimally Invasive Glaucoma Surgery (Migs) : Cynthia V. Verzosa, MD, Dpbo, MSCCynthia VerzosaNo ratings yet
- CVV Tafluprost S LectureDocument50 pagesCVV Tafluprost S LectureCynthia VerzosaNo ratings yet
- Pre-Op Preparations For Healthier Blebs FinalDocument34 pagesPre-Op Preparations For Healthier Blebs FinalCynthia VerzosaNo ratings yet
- Practical Automated Visual Field Interpretation: Cynthia V. Verzosa, MD, Dpbo, MSC On Behalf of TheDocument41 pagesPractical Automated Visual Field Interpretation: Cynthia V. Verzosa, MD, Dpbo, MSC On Behalf of TheCynthia VerzosaNo ratings yet
- Glaucoma after Trauma: A Review of Pathophysiology and ManagementDocument44 pagesGlaucoma after Trauma: A Review of Pathophysiology and ManagementCynthia VerzosaNo ratings yet
- HIKVISION Pricelist SEPTEMBER 2018Document17 pagesHIKVISION Pricelist SEPTEMBER 2018PRANOTONo ratings yet
- The CorneaDocument57 pagesThe CorneatutsimundiNo ratings yet
- Sanet - ST The - Color.management - Handbook.for - Visual.effects - ArtistsDocument251 pagesSanet - ST The - Color.management - Handbook.for - Visual.effects - ArtistssquidxpNo ratings yet
- Thesis Rodulfo Eye Re (Formation) Integration of Architecture and Vision Therapy For The VisualimpairedDocument69 pagesThesis Rodulfo Eye Re (Formation) Integration of Architecture and Vision Therapy For The VisualimpairedPierre RodulfoNo ratings yet
- Dwnload Full Experience Music 4th Edition Charlton Solutions Manual PDFDocument33 pagesDwnload Full Experience Music 4th Edition Charlton Solutions Manual PDFsymmetryairgunu9qj100% (14)
- B Scan Ultrasonography01Document54 pagesB Scan Ultrasonography01dr samreen arif50% (2)
- IP UT 1 NotesDocument19 pagesIP UT 1 NotesKartik SomaniNo ratings yet
- CRSTE0418 - Fundamentals - Holladlay - Kappa AngleDocument3 pagesCRSTE0418 - Fundamentals - Holladlay - Kappa AngleDickyStevanoZukhriNo ratings yet
- Characteristics & Classification of Living Organisms 3 MSDocument7 pagesCharacteristics & Classification of Living Organisms 3 MSRameenNo ratings yet
- Feeling Through Sight Zooming in Zooming OutDocument19 pagesFeeling Through Sight Zooming in Zooming OutYUE ZHONGNo ratings yet
- Makalah Company Profile Group-6Document11 pagesMakalah Company Profile Group-6Amoysz QheabotNo ratings yet
- Medical Physics Ch14 Electrical Technology & Ch15 OpticsDocument47 pagesMedical Physics Ch14 Electrical Technology & Ch15 OpticsAbdullahi Mohamed IsakNo ratings yet
- Guide to Cataract Surgery RecoveryDocument16 pagesGuide to Cataract Surgery Recoverydokumen kuNo ratings yet
- Diagnosis and Management of Posterior Intraocular Lens Dislocation with IOL Exchange to Iris Claw RetropupillaryDocument13 pagesDiagnosis and Management of Posterior Intraocular Lens Dislocation with IOL Exchange to Iris Claw Retropupillarymemmuse95No ratings yet
- Physics NotesDocument43 pagesPhysics NotesRaj ManovaNo ratings yet
- Light-The Human and The Colourful WorldDocument11 pagesLight-The Human and The Colourful WorldTapas BanerjeeNo ratings yet
- Fundamentals of Pharmacology For Veterinary TechniciansDocument12 pagesFundamentals of Pharmacology For Veterinary TechniciansHuma Hameed DogarNo ratings yet
- 3D Printed Digital Night Vision (The Openscope) : InstructablesDocument53 pages3D Printed Digital Night Vision (The Openscope) : InstructablesAdven TuresNo ratings yet
- 129 Accommodative EsotropiaDocument6 pages129 Accommodative EsotropiakarenafiafiNo ratings yet
- L16.2 OPHTHA Ocular Motility (Nov1622)Document5 pagesL16.2 OPHTHA Ocular Motility (Nov1622)Erald PaderangaNo ratings yet
- Soal Refraksi AaoDocument4 pagesSoal Refraksi Aaoria mutiaraNo ratings yet
- Dwnload Full Physics 5th Edition Walker Solutions Manual PDFDocument36 pagesDwnload Full Physics 5th Edition Walker Solutions Manual PDFmarcusquyepv100% (10)
- MataDocument20 pagesMataFahrin AhmadNo ratings yet
- Notes - Notes - Ophthalmology PDFDocument30 pagesNotes - Notes - Ophthalmology PDFRumana Ali100% (2)
- Medical RetinaDocument170 pagesMedical Retinacristina grigoreNo ratings yet
- Chapter Two Human in HCIDocument36 pagesChapter Two Human in HCIEbisa EdessaNo ratings yet
- Ophthalmology Card AnswersDocument29 pagesOphthalmology Card AnswersRaihan MahmudNo ratings yet
- The History of Animals - by AristotleDocument17 pagesThe History of Animals - by Aristotledenunciaambev2023No ratings yet
- 2.RGP Corneal LensDocument13 pages2.RGP Corneal LensAlpaNo ratings yet
- Biology Communication NotesDocument19 pagesBiology Communication NotesjobinNo ratings yet