You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Case Study #31: Nutrition Support in Sepsis and Morbid ObesityDocument24 pagesCase Study #31: Nutrition Support in Sepsis and Morbid ObesityCuteScribd100% (1)
- GHA 2020 Changes L Training MaterialDocument42 pagesGHA 2020 Changes L Training MaterialJULIUS TIBERIONo ratings yet
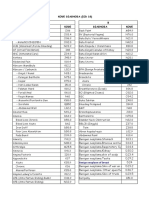
- Diagnosa Icd 10 SilDocument51 pagesDiagnosa Icd 10 SilinayaNo ratings yet
- K. Park 26th Edition - New UpdatesDocument191 pagesK. Park 26th Edition - New UpdatesSMO Bokaro38% (16)
- Post Mortem CareDocument1 pagePost Mortem CareElishah CaprichoNo ratings yet
- Roy ReferatDocument8 pagesRoy ReferatFadel Aneuk NanggroeNo ratings yet
- Vitamin B (Much As People Refer To Vitamin C or Vitamin D)Document16 pagesVitamin B (Much As People Refer To Vitamin C or Vitamin D)Aisha MohamedNo ratings yet
- THE ROOTS OF INTERNATIONAL DERMATOLOGY: A Historical TabulationDocument7 pagesTHE ROOTS OF INTERNATIONAL DERMATOLOGY: A Historical TabulationAisha MohamedNo ratings yet
- Vitamin B (Much As People Refer To Vitamin C or Vitamin D)Document16 pagesVitamin B (Much As People Refer To Vitamin C or Vitamin D)Aisha MohamedNo ratings yet
- Dr+Sewillam+Clinical+Book+Full+by+دكتور الا ربعDocument351 pagesDr+Sewillam+Clinical+Book+Full+by+دكتور الا ربعAisha MohamedNo ratings yet
- Thyroid Gland: Mr. Tarig AbbasDocument28 pagesThyroid Gland: Mr. Tarig AbbasAisha MohamedNo ratings yet
- Jurnal Tinea Unguium - 1Document6 pagesJurnal Tinea Unguium - 1FazaKhilwanAmnaNo ratings yet
- Chick ListDocument1 pageChick ListMohammed ElhashimiNo ratings yet
- Miopatías Inflamatorias IdiopáticasDocument14 pagesMiopatías Inflamatorias IdiopáticasGerarNo ratings yet
- Case Study 7th July 2021Document2 pagesCase Study 7th July 2021sivakamasundari pichaipillaiNo ratings yet
- Adapted From Background To British and American CulturesDocument5 pagesAdapted From Background To British and American CulturesVăn phú NguyễnNo ratings yet
- Corona Virus InfographicDocument1 pageCorona Virus Infographicapi-510312435No ratings yet
- Invitation Letter With Written Pledge EnglishDocument2 pagesInvitation Letter With Written Pledge EnglishADA ADA SAJANo ratings yet
- Ait Nejm 2020Document9 pagesAit Nejm 2020Ahmed JallouliNo ratings yet
- Master The Guides Ch1Document26 pagesMaster The Guides Ch1workcovervictim8242No ratings yet
- Pediatric Concept MapDocument7 pagesPediatric Concept Mapapi-508020518No ratings yet
- Icd 10Document8 pagesIcd 10Ilun DonaldcocainNo ratings yet
- Lassa Fever Fact SheetDocument2 pagesLassa Fever Fact SheetOfowu OmohohwoNo ratings yet
- Niemann Pick DiseaseDocument3 pagesNiemann Pick Diseaseडा. सत्यदेव त्यागी आर्यNo ratings yet
- Erythrocyte Sedimentation Rate: Definition DeterminationDocument3 pagesErythrocyte Sedimentation Rate: Definition DeterminationAnusuya SNo ratings yet
- Pathophysiology Format: Predisposing Factors Precipitating Factors (Contributing) (Triggering)Document2 pagesPathophysiology Format: Predisposing Factors Precipitating Factors (Contributing) (Triggering)AyaBasilioNo ratings yet
- Assignment Solutions - 254Document5 pagesAssignment Solutions - 254Prof OliviaNo ratings yet
- Hyperthermia Augments Neoadjuvant Chemotherapy On Breast Carcinoma - A Case ReportDocument3 pagesHyperthermia Augments Neoadjuvant Chemotherapy On Breast Carcinoma - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- TUBERCULOSISDocument4 pagesTUBERCULOSISLâm NguyễnNo ratings yet
- Daftar Kode Icd 10Document5 pagesDaftar Kode Icd 10erliNo ratings yet
- Who Pneu Im Pgi ProtocolDocument2 pagesWho Pneu Im Pgi ProtocolRoxanneGailBigcasGoleroNo ratings yet
- LB1 SimpusDocument47 pagesLB1 SimpusChoririn Erick GumilarNo ratings yet
- Worm InfestationDocument1 pageWorm InfestationMRS CHAKRAPANINo ratings yet
- 2nd MAPEH 3Document2 pages2nd MAPEH 3Edmar MejiaNo ratings yet
- Signs and Symptoms of Pancreatic Cancer Fact Sheet Dec 2014Document6 pagesSigns and Symptoms of Pancreatic Cancer Fact Sheet Dec 2014Nus EuNo ratings yet