You might also like
- Hook worms: Causes, Symptoms, Diagnosis and TreatmentDocument12 pagesHook worms: Causes, Symptoms, Diagnosis and TreatmentIbrahim Mahmoud Ali100% (1)
- Nematodes LabDocument57 pagesNematodes LabAlaa ZiyadNo ratings yet
- 3.b.coli, Crypt, Cyclo, Iso, Sarco, Microsp, Acnth, NaegDocument86 pages3.b.coli, Crypt, Cyclo, Iso, Sarco, Microsp, Acnth, NaegPallavi Uday NaikNo ratings yet
- Lecture 6 2023Document16 pagesLecture 6 2023ayaessam392002No ratings yet
- Everything You Need to Know About NematodesDocument116 pagesEverything You Need to Know About NematodesKateNo ratings yet
- Micro-Para Practical Exam ReviewerDocument8 pagesMicro-Para Practical Exam ReviewerRA TranceNo ratings yet
- Lecture 3 - Intestinal Nematodes, Trematod Cestodes of Medical ImportanceDocument118 pagesLecture 3 - Intestinal Nematodes, Trematod Cestodes of Medical ImportanceshwtybeNo ratings yet
- Lecture 7 Nematodes Part 2 New 2023Document19 pagesLecture 7 Nematodes Part 2 New 2023ayaessam392002No ratings yet
- Nematodes: 2. Enterobius VermicularisDocument2 pagesNematodes: 2. Enterobius VermicularisCia QuebecNo ratings yet
- Trematodes and NemahelminthesDocument6 pagesTrematodes and NemahelminthesEvelyn TingNo ratings yet
- Schistosomapptdrsomesh2015 151217103710Document39 pagesSchistosomapptdrsomesh2015 151217103710Al Karkab آل كركابNo ratings yet
- Medicine Lec.11 - HelminthsDocument39 pagesMedicine Lec.11 - Helminths7fefdfbea1No ratings yet
- Petrache, Joseph Dacanay, Gilian Medina, Julius Co, Kenneth Jr. Corcelles, KevinDocument120 pagesPetrache, Joseph Dacanay, Gilian Medina, Julius Co, Kenneth Jr. Corcelles, KevinGilian Dacanay100% (2)
- Microbiology - ParasitologyDocument34 pagesMicrobiology - ParasitologySasi DharanNo ratings yet
- General Characters of Nematodes: Cylindrical Cuticle. SeparateDocument18 pagesGeneral Characters of Nematodes: Cylindrical Cuticle. SeparateAyop KhNo ratings yet
- Nematodes and Cestodes OutlineDocument6 pagesNematodes and Cestodes OutlineFarlogy80% (5)
- Hook worms: Ancylostoma duodenale and Necator americanusDocument21 pagesHook worms: Ancylostoma duodenale and Necator americanusLisa Hidayati DainirNo ratings yet
- Trematodes 2Document37 pagesTrematodes 2Akanksha BaireddyNo ratings yet
- Strongyloides Stercoralis: Faecal Like CylinderDocument18 pagesStrongyloides Stercoralis: Faecal Like CylinderAyop KhNo ratings yet
- 012-Trichuris Trichiura and EnterobiusDocument15 pages012-Trichuris Trichiura and EnterobiusAyop KhNo ratings yet
- Parasites of Medical ImportanceDocument9 pagesParasites of Medical ImportanceKimberly RampersadNo ratings yet
- Parasitic Flatworms and Tapeworms Classification and CharacteristicsDocument54 pagesParasitic Flatworms and Tapeworms Classification and CharacteristicsMewa MahartaNo ratings yet
- Helminths Part1Document125 pagesHelminths Part1monica_gallardo_24No ratings yet
- NEMATODESDocument20 pagesNEMATODESLycah Jyde PechuancoNo ratings yet
- SchistosomesDocument12 pagesSchistosomesMORDENO, JOHN GABRIEL O. SCINo ratings yet
- Parasitology Helmit Print OutDocument64 pagesParasitology Helmit Print Outprabad dunusingheNo ratings yet
- Key Points of Chapter 14-20Document3 pagesKey Points of Chapter 14-20Cecil AguilarNo ratings yet
- Micro ParasitologyDocument5 pagesMicro ParasitologyPlzstudylav SyedNo ratings yet
- HookwormsDocument42 pagesHookwormsGiovanna AlguNo ratings yet
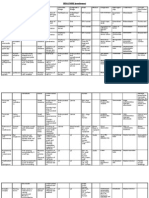
- Topnotch Parasitology Super Table by DR - Yns PereyraDocument50 pagesTopnotch Parasitology Super Table by DR - Yns PereyraRochelle Joyce AradoNo ratings yet
- Paramarch15 1Document39 pagesParamarch15 1Jerryco BalasterosNo ratings yet
- EntamoebaDocument94 pagesEntamoebaAtlas AstreaNo ratings yet
- ProtozoologyDocument28 pagesProtozoologyStella Agatha WidjajaNo ratings yet
- Parasite Project BIOLOGY EditedDocument21 pagesParasite Project BIOLOGY EditedPadma CharanNo ratings yet
- Infeksi Cacing Yang Penting Di IndonesiaDocument44 pagesInfeksi Cacing Yang Penting Di IndonesiaHendricNo ratings yet
- 007-General Characters of Cestodes + DiphyllobothriumDocument15 pages007-General Characters of Cestodes + DiphyllobothriumAyop KhNo ratings yet
- Parasitic Infection in GI TractDocument123 pagesParasitic Infection in GI TractUtami HandayaniNo ratings yet
- Hook worms: Ancylostoma duodenale and Necator americanusDocument20 pagesHook worms: Ancylostoma duodenale and Necator americanusMladen Vasiljević100% (1)
- hookworm (1)747731995Document18 pageshookworm (1)747731995mittal.shubham0007No ratings yet
- ClinPara FlagellatesDocument10 pagesClinPara FlagellatesStephen YorNo ratings yet
- Smallpox A Dead Disease: Dr.T.V.Rao MDDocument46 pagesSmallpox A Dead Disease: Dr.T.V.Rao MDshravaniNo ratings yet
- PMC503 Parasitology Nematoda 1 2022Document33 pagesPMC503 Parasitology Nematoda 1 2022Adam DiabNo ratings yet
- PMC503 Parasitology Nematoda 1 2022Document33 pagesPMC503 Parasitology Nematoda 1 2022Adam DiabNo ratings yet
- Six Flukes. TrematodeDocument106 pagesSix Flukes. TrematodeCherenet TomaNo ratings yet
- The Intestinal NematodesDocument107 pagesThe Intestinal Nematodesblue_blooded23100% (1)
- Parasitology NotesDocument5 pagesParasitology NotesAndriaNo ratings yet
- 8-Trematodes Ibrahim2016Document35 pages8-Trematodes Ibrahim2016Buntukazi MapamelaNo ratings yet
- Ancy Lost OmaDocument41 pagesAncy Lost OmaMuhmmad TahaNo ratings yet
- Parasite InfectionsDocument45 pagesParasite InfectionsAbdullah AlkharsNo ratings yet
- (AGUE) : Transmitted by A Mosquito Bite Causative Agent: P.: Malignant Tertian P. Benign Tertian PDocument27 pages(AGUE) : Transmitted by A Mosquito Bite Causative Agent: P.: Malignant Tertian P. Benign Tertian PEbiNo ratings yet
- Parasitology: Is The Study of ParasitesDocument51 pagesParasitology: Is The Study of ParasitesMarz ALNo ratings yet
- Schistosoma haematobium InfectionDocument30 pagesSchistosoma haematobium InfectionRaihanur KiranNo ratings yet
- Parasaitology HelminthDocument139 pagesParasaitology Helminthkidus asnNo ratings yet
- PARA Class NematodaDocument106 pagesPARA Class NematodaKaycee AyoNo ratings yet
- Infeksi Cacing Yang Penting di IndonesiaDocument44 pagesInfeksi Cacing Yang Penting di IndonesiaLulu MafrudhotulNo ratings yet
- 016 Trichinella Spiralis DracunculusDocument14 pages016 Trichinella Spiralis DracunculusAyop KhNo ratings yet
- Par201 S1lab4 Midterm Phamids Aphasmids PDFDocument27 pagesPar201 S1lab4 Midterm Phamids Aphasmids PDFHanna Alyssa Grace DimarananNo ratings yet
- 911 Pigeon Disease & Treatment Protocols!From Everand911 Pigeon Disease & Treatment Protocols!Rating: 4 out of 5 stars4/5 (1)
- Proceedings of the First International Congress of Parasitology: Roma, 21-26 September 1964From EverandProceedings of the First International Congress of Parasitology: Roma, 21-26 September 1964Augusto CorradettiNo ratings yet
- 017 Wuchereria BrugiaDocument21 pages017 Wuchereria BrugiaAyop KhNo ratings yet
- 018 Loa Loa OnchocercaDocument19 pages018 Loa Loa OnchocercaAyop KhNo ratings yet
- General Characters of Nematodes: Cylindrical Cuticle. SeparateDocument18 pagesGeneral Characters of Nematodes: Cylindrical Cuticle. SeparateAyop KhNo ratings yet
- Strongyloides Stercoralis: Faecal Like CylinderDocument18 pagesStrongyloides Stercoralis: Faecal Like CylinderAyop KhNo ratings yet
- 016 Trichinella Spiralis DracunculusDocument14 pages016 Trichinella Spiralis DracunculusAyop KhNo ratings yet
- Ancylostoma Duodenale: What Happens When Infective Filariform Larva of Penetrates Human Skin ?Document16 pagesAncylostoma Duodenale: What Happens When Infective Filariform Larva of Penetrates Human Skin ?Ayop KhNo ratings yet
- 009-Echinococcus, Multiceps CombinedDocument19 pages009-Echinococcus, Multiceps CombinedAyop KhNo ratings yet
- 007-General Characters of Cestodes + DiphyllobothriumDocument15 pages007-General Characters of Cestodes + DiphyllobothriumAyop KhNo ratings yet
- 012-Trichuris Trichiura and EnterobiusDocument15 pages012-Trichuris Trichiura and EnterobiusAyop KhNo ratings yet
- 010-H.nana, Diminuta & Caninum - Nana, Diminuta & CaninumDocument13 pages010-H.nana, Diminuta & Caninum - Nana, Diminuta & CaninumAyop KhNo ratings yet
- Taenia Causes Taeniasis and CysticercosisDocument16 pagesTaenia Causes Taeniasis and CysticercosisAyop KhNo ratings yet
- Opara Et AlDocument10 pagesOpara Et AlAntoninus HengkyNo ratings yet
- 6 Tissue Terrains ColorDocument1 page6 Tissue Terrains Colorஆ.க.கோ. இராஜேஷ்வரக் கோன்No ratings yet
- AllopurinolDocument1 pageAllopurinolMelissa VilarNo ratings yet
- Stretta Patint Info Sheet Rev Oct 2018Document6 pagesStretta Patint Info Sheet Rev Oct 2018Stamatis KourtisNo ratings yet
- Test Bank For Human Diseases 3rd Edition NeighborsDocument13 pagesTest Bank For Human Diseases 3rd Edition Neighborsdenisedanielsbkgqyzmtr100% (24)
- Act 259 Indecent Advertisements Act 1953Document10 pagesAct 259 Indecent Advertisements Act 1953Adam Haida & CoNo ratings yet
- 28 Biochemic CombinationDocument6 pages28 Biochemic CombinationMustafa AliNo ratings yet
- (Microbiology) Microbiological Food PoisoningDocument72 pages(Microbiology) Microbiological Food Poisoningamin100% (1)
- Department of Health: Adolescent and Youth Health and Development Program (AYHDP)Document37 pagesDepartment of Health: Adolescent and Youth Health and Development Program (AYHDP)Apol PenNo ratings yet
- Biology 9th Solving A Biological ProblemDocument5 pagesBiology 9th Solving A Biological Problemmhussainshigri786No ratings yet
- Tugas Bahasa Inggris 2Document6 pagesTugas Bahasa Inggris 2yuly sukmawatiNo ratings yet
- Nursing Care Plan DiarrheaDocument2 pagesNursing Care Plan Diarrheaderic95% (43)
- GMR-Service PPT (2018-19)Document19 pagesGMR-Service PPT (2018-19)Sanjeet GaurNo ratings yet
- Cme Fast ScanDocument25 pagesCme Fast Scannirmal raj100% (1)
- Nursing Care Plan TB MeningitisDocument2 pagesNursing Care Plan TB Meningitisderic74% (19)
- Foster ShawnDocument32 pagesFoster ShawnSuman DeyNo ratings yet
- How To Overcome Depression PDFDocument9 pagesHow To Overcome Depression PDFjakirNo ratings yet
- Monitoring Tool For Evluation of Performance of The Staff Nurse During Admission, Transfer & Discharge of The PatientDocument12 pagesMonitoring Tool For Evluation of Performance of The Staff Nurse During Admission, Transfer & Discharge of The Patientmahbuburrahim9553No ratings yet
- Papaya - An Innovative Raw Material For Food and Pharmaceutical Processing IndustryDocument8 pagesPapaya - An Innovative Raw Material For Food and Pharmaceutical Processing IndustryNurul FaizaahNo ratings yet
- Disorders of The Digestive System AssignmentDocument2 pagesDisorders of The Digestive System Assignmentsanjay kajal100% (1)
- Research Abstracts On NutritionDocument172 pagesResearch Abstracts On NutritionKulwinder KaurNo ratings yet
- (Pediaii) - 021 - Disorders of The Respiratory TractDocument17 pages(Pediaii) - 021 - Disorders of The Respiratory TractdoktoraronaNo ratings yet
- Schizoobsessive Spectrum Disorders An UpdateDocument15 pagesSchizoobsessive Spectrum Disorders An UpdateRubiNo ratings yet
- General Climaco National High School General Climaco, Toledo City Diagnostic Exam (Mapeh 8)Document3 pagesGeneral Climaco National High School General Climaco, Toledo City Diagnostic Exam (Mapeh 8)blessyroseNo ratings yet
- Red Cross CPR Class InfoDocument3 pagesRed Cross CPR Class Infoapi-124274210No ratings yet
- Richardson 86yoF Afib on pradaxa admitted with hypotension and night sweatsDocument3 pagesRichardson 86yoF Afib on pradaxa admitted with hypotension and night sweatsMichaelNo ratings yet
- PPT Inggris DMDocument9 pagesPPT Inggris DMtria WidiastutiNo ratings yet
- MAHARASHTRA UNIVERSITY OF HEALTH SCIENCES SYLLABUSDocument7 pagesMAHARASHTRA UNIVERSITY OF HEALTH SCIENCES SYLLABUSEjaj BuzrukNo ratings yet
- The Many Benefits of Hydrogen PeroxideDocument9 pagesThe Many Benefits of Hydrogen PeroxideRedza100% (7)
- Chicken Pox ReportDocument25 pagesChicken Pox ReportDyanne BautistaNo ratings yet