You might also like
- What's New 20dec2022 ( (Autorecovered-310036581311017056) )Document19 pagesWhat's New 20dec2022 ( (Autorecovered-310036581311017056) )Abir HarmouchNo ratings yet
- NavelbinDocument48 pagesNavelbinanang atmojoNo ratings yet
- EsmoMetastatic Colorectal CancerDocument41 pagesEsmoMetastatic Colorectal CancerrafatrujNo ratings yet
- Breast Cancer Treatment and Surveillance GuideDocument3 pagesBreast Cancer Treatment and Surveillance GuideAneeshNo ratings yet
- AFib WarfarinVsNOACsDocument2 pagesAFib WarfarinVsNOACsalpha wolfNo ratings yet
- Olmos. Secuencia Novartis 2023 H12ODocument36 pagesOlmos. Secuencia Novartis 2023 H12ODavid OlmosNo ratings yet
- TRIALSDocument4 pagesTRIALSusmleusmle86No ratings yet
- 1 - Intro - E.Castro Guidelines Webinar ProstateDocument12 pages1 - Intro - E.Castro Guidelines Webinar Prostateveaceslav coscodanNo ratings yet
- AlzheimerDocument163 pagesAlzheimerferreira.laurinda7995100% (1)
- 13 00 - 14 00 Sandra Franco Almuerzo Simposio MSD TNCB Inmunoterapia - MedellinDocument14 pages13 00 - 14 00 Sandra Franco Almuerzo Simposio MSD TNCB Inmunoterapia - Medellininfo7615No ratings yet
- Oncology Outpatient Daily Report: Friday, December 7 2018Document16 pagesOncology Outpatient Daily Report: Friday, December 7 2018Rebeka Anastasia MarpaungNo ratings yet
- Oncology Outpatient Daily Report: Monday, November 12 2018Document18 pagesOncology Outpatient Daily Report: Monday, November 12 2018Rebeka Anastasia MarpaungNo ratings yet
- Esmooesphago Gastic CancerDocument32 pagesEsmooesphago Gastic CancerrafatrujNo ratings yet
- Nicu Over SheetDocument1 pageNicu Over SheetDoc Ahmad NaseerNo ratings yet
- Materi PKB 2022-RevisiDocument27 pagesMateri PKB 2022-RevisiNatzirbuttoNo ratings yet
- December 12Document12 pagesDecember 12Reda SoNo ratings yet
- Algorithm for managing anticoagulant therapy in Acute Coronary SyndromeDocument46 pagesAlgorithm for managing anticoagulant therapy in Acute Coronary SyndromeCresti Chandra PradeltaNo ratings yet
- Cardiac Troponin: Prof. Adi Koesoema AmanDocument58 pagesCardiac Troponin: Prof. Adi Koesoema Amanbudi darmantaNo ratings yet
- TCT Template Title 30 PT Bold Arial: Ongoing Clinical Trials and The Future of LAACDocument23 pagesTCT Template Title 30 PT Bold Arial: Ongoing Clinical Trials and The Future of LAACCesar CuellarNo ratings yet
- 1 - UK Lamuno Plus BrochureDocument2 pages1 - UK Lamuno Plus BrochurePhyo WaiNo ratings yet
- "Adjunctive Therapy" Non ST Segment Elevation ACS: DR M R Thomas King's College Hospital. Advanced Angioplasty 2002Document42 pages"Adjunctive Therapy" Non ST Segment Elevation ACS: DR M R Thomas King's College Hospital. Advanced Angioplasty 2002usfcardsNo ratings yet
- Colorectal Cancer File1Document1 pageColorectal Cancer File1Ramez AntakiaNo ratings yet
- Doctor's Order SampleDocument3 pagesDoctor's Order SampleXerxes DejitoNo ratings yet
- PocketCard UPDATE2013 EnglishDocument2 pagesPocketCard UPDATE2013 EnglishTowhidulIslamNo ratings yet
- T3 - Pack Code DetailsDocument302 pagesT3 - Pack Code DetailskiranNo ratings yet
- Komparasi Lyra X1Document1 pageKomparasi Lyra X1Ikhsan FakhurroziNo ratings yet
- BK VirusDocument59 pagesBK Virusعبدالحافظ مامونNo ratings yet
- Linfoma y Leumicias UntDocument77 pagesLinfoma y Leumicias UntJAIME YOSHIMAR MENDEZ PEREZNo ratings yet
- High Sensitivity Cardiac Troponin I and T Assay Analytical Characteristics Designated by Manufacturer v122019Document4 pagesHigh Sensitivity Cardiac Troponin I and T Assay Analytical Characteristics Designated by Manufacturer v122019MiguelNo ratings yet
- GLI meeting focuses on DST diagnostic technologies for tuberculosis diagnosisDocument30 pagesGLI meeting focuses on DST diagnostic technologies for tuberculosis diagnosisWawan BahmidNo ratings yet
- Curriculum Vitae and Radiation Therapy for Gynecologic CancerDocument31 pagesCurriculum Vitae and Radiation Therapy for Gynecologic CancerpisangphoeNo ratings yet
- Saito 2006Document8 pagesSaito 2006cindyNo ratings yet
- Trauma Male A: General Surgery: Team I Dr. Tamani/Lingan/Aguisanda/Baculi/Casco/ BulusanDocument7 pagesTrauma Male A: General Surgery: Team I Dr. Tamani/Lingan/Aguisanda/Baculi/Casco/ BulusanLuis PadillaNo ratings yet
- RNL DruDocument1 pageRNL DruLanaAmerieNo ratings yet
- Cardiology USMLE 2CK (Cardio Clinical Care) Flashcards - MemorangDocument4 pagesCardiology USMLE 2CK (Cardio Clinical Care) Flashcards - MemorangMohamed Abbas0% (2)
- New Agents On The Horizon: Implications For Phase I, Ii & Iii Trials DNA Repair and PARP InhibitorsDocument18 pagesNew Agents On The Horizon: Implications For Phase I, Ii & Iii Trials DNA Repair and PARP InhibitorsVito DamascoNo ratings yet
- Updated Management of HypertriglyceridaemiaDocument32 pagesUpdated Management of Hypertriglyceridaemiaanon_701937590No ratings yet
- ONCOLOGY OUTPATIENT DAILY REPORT RECAPDocument12 pagesONCOLOGY OUTPATIENT DAILY REPORT RECAPRebeka Anastasia MarpaungNo ratings yet
- ALL Protocol-Feb 19, 2016Document26 pagesALL Protocol-Feb 19, 2016Mohammed HaiderNo ratings yet
- A22M0163DR - ArponDocument7 pagesA22M0163DR - ArponAnton CornelNo ratings yet
- Oncology Outpatient Daily Report RecapDocument8 pagesOncology Outpatient Daily Report RecapRebeka Anastasia MarpaungNo ratings yet
- Cervix - Presente y Futuro Del Manejo Quirúrgico - Mario LeitaoDocument51 pagesCervix - Presente y Futuro Del Manejo Quirúrgico - Mario Leitaoinfo7615No ratings yet
- Pediatric LeukemiasDocument42 pagesPediatric LeukemiasslyfoxkittyNo ratings yet
- Tuberculosis Background: Causes, Transmission, Prevalence and TreatmentDocument11 pagesTuberculosis Background: Causes, Transmission, Prevalence and TreatmentSanju SNo ratings yet
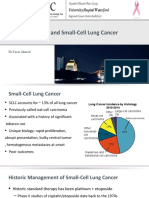
- Immunotherapy and Small-Cell Lung CancerDocument33 pagesImmunotherapy and Small-Cell Lung CancerYasar HammorNo ratings yet
- NCGM Price List - (Rainbow H)Document6 pagesNCGM Price List - (Rainbow H)Yatharath BhardwajNo ratings yet
- Inventaris Alat Medis 2020Document9 pagesInventaris Alat Medis 2020wahyuwiarsoNo ratings yet
- PASIEN DIGESTIF OHO - 2 Januari 2019 (R1, R2B, R3, R4B)Document2 pagesPASIEN DIGESTIF OHO - 2 Januari 2019 (R1, R2B, R3, R4B)Wahyu Hendra PrabowoNo ratings yet
- Esmo 2020 Hendriks 021020Document27 pagesEsmo 2020 Hendriks 021020TaloipaNo ratings yet
- Template UmumDocument2 pagesTemplate UmumsafaridikaNo ratings yet
- Cluj - LRCL PDFDocument28 pagesCluj - LRCL PDFRăzvan Florin ConstantinNo ratings yet
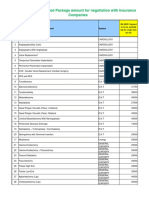
- IMA NHB Suggested Package Amount For Negotiation With Insurance CompaniesDocument5 pagesIMA NHB Suggested Package Amount For Negotiation With Insurance Companiesmonikparmar1No ratings yet
- Health Sector Response To COVID-19Document8 pagesHealth Sector Response To COVID-19ANUP GAUTAMNo ratings yet
- PDUI - Final - DRDocument28 pagesPDUI - Final - DRbio rizkimaulanaNo ratings yet
- CABG Beats PCI for Left Main DiseaseDocument44 pagesCABG Beats PCI for Left Main DiseaseAnindyaSarkar100% (1)
- Early Treatment of Breast CancerDocument31 pagesEarly Treatment of Breast CancerZaayaNo ratings yet
- CaRectum (DR - Soetamto Wibowo)Document25 pagesCaRectum (DR - Soetamto Wibowo)Elandha Putri100% (1)
- Immune Thrombocytopenia Patient CaseDocument27 pagesImmune Thrombocytopenia Patient Caseapi-648595816No ratings yet
- Flight For Life 81M.01 Mechanical Ventilation 2022-07-01Document4 pagesFlight For Life 81M.01 Mechanical Ventilation 2022-07-01Bryan WinchellNo ratings yet
- Hypofractionated and Stereotactic Radiation Therapy: A Practical GuideFrom EverandHypofractionated and Stereotactic Radiation Therapy: A Practical GuideOrit Kaidar-PersonNo ratings yet
- DRUGDocument13 pagesDRUGReniNo ratings yet
- Small Animal Clinical Pharmacology and TherapeuticsDocument820 pagesSmall Animal Clinical Pharmacology and TherapeuticsDanielle GodoyNo ratings yet
- 2022 - July - 25 - Drug Price Reference IndexDocument45 pages2022 - July - 25 - Drug Price Reference Indexkhara teanoNo ratings yet
- Suctioning Procedure ChecklistDocument2 pagesSuctioning Procedure ChecklistRamanujam Sekar67% (3)
- NPH Insulin NPHDocument1 pageNPH Insulin NPHE100% (1)
- MetforminDocument5 pagesMetforminAyeshaNo ratings yet
- O2 ModalitiesDocument49 pagesO2 ModalitiesVyklyn Testa0% (1)
- PCNE Classification For Drug-Related Problems V9.1 - Page 1Document10 pagesPCNE Classification For Drug-Related Problems V9.1 - Page 1Selinda Anggia DeviNo ratings yet
- Mesoglow y MesoliftDocument2 pagesMesoglow y MesoliftPablo BaudinoNo ratings yet
- Aminophylline GuidelinesDocument2 pagesAminophylline GuidelinesA. Shamshir A. MoktiNo ratings yet
- Factors Modifying Drug ActionsDocument3 pagesFactors Modifying Drug ActionsDAMBALE0% (1)
- Buffer StockDocument26 pagesBuffer Stockfatha_87No ratings yet
- Gautam Poudel: AcademicsDocument2 pagesGautam Poudel: AcademicsGautam PoudelNo ratings yet
- Kuhn Et Al-2017-Journal of The European Academy of Dermatology and VenereologyDocument16 pagesKuhn Et Al-2017-Journal of The European Academy of Dermatology and VenereologyShree ShresthaNo ratings yet
- Rabia Parveen Mangi: LecturerDocument8 pagesRabia Parveen Mangi: LecturerQalab HussainNo ratings yet
- What Is Clinical Research?: 5520 Lyndon B Johnson FWY, Suite 100 Dallas, TX 75240Document3 pagesWhat Is Clinical Research?: 5520 Lyndon B Johnson FWY, Suite 100 Dallas, TX 75240Stacey HillNo ratings yet
- Psychiatric Nursing PrelimDocument7 pagesPsychiatric Nursing Prelimalexancog456No ratings yet
- PT Global Onkolab Farma: Stock Detail Period 420.00Document6 pagesPT Global Onkolab Farma: Stock Detail Period 420.00Toni FatoniNo ratings yet
- Classic Laryngeal Mask Airway Insertion With Laryngoscope Mcgrath and Macintosh: A Case SeriesDocument3 pagesClassic Laryngeal Mask Airway Insertion With Laryngoscope Mcgrath and Macintosh: A Case SeriesYeyen AgustinNo ratings yet
- Small Molecule Drug Discovery PresentationDocument11 pagesSmall Molecule Drug Discovery PresentationRohitNo ratings yet
- Module 1 ReviewDocument27 pagesModule 1 ReviewAmanda LabateNo ratings yet
- Daftar Barang Astro 03 April 2023Document35 pagesDaftar Barang Astro 03 April 2023ngawi farmasiNo ratings yet
- HIV and Its TreatmentDocument24 pagesHIV and Its Treatmentaathira_kNo ratings yet
- Kolkata PPN Hospital - Procedure ListDocument16 pagesKolkata PPN Hospital - Procedure ListMohan KumarNo ratings yet
- Poisoning PPT Nursing FoundationDocument16 pagesPoisoning PPT Nursing FoundationMahimaNo ratings yet
- Ranx 500 MGDocument4 pagesRanx 500 MGChetan L. PujaraNo ratings yet
- Premarin Drug StudyDocument8 pagesPremarin Drug StudyjanNo ratings yet
- Antibiotic Dosing Challenges in CKDDocument11 pagesAntibiotic Dosing Challenges in CKDChiranjib BagchiNo ratings yet
- Dry SocketDocument1 pageDry SocketFaizel SyedNo ratings yet
- Procedure For Leech TherapyDocument5 pagesProcedure For Leech TherapyAlin LabauNo ratings yet