You might also like
- Bacterial VaginosisDocument20 pagesBacterial VaginosisTum M. TansakulNo ratings yet
- Antenatal Info Booklet Intuitive BirthDocument32 pagesAntenatal Info Booklet Intuitive Birthapi-223713414No ratings yet
- Tuberculosis: Therapeutics IIDocument54 pagesTuberculosis: Therapeutics IIdstu20No ratings yet
- Pulmonary Tuberculosis (PTB)Document6 pagesPulmonary Tuberculosis (PTB)carls burg a. resurreccion100% (2)
- Pathogenesis of TBDocument82 pagesPathogenesis of TBanto mathewNo ratings yet
- A Presentation On-: Dr. Nikhil Oza Intern BvdumcDocument43 pagesA Presentation On-: Dr. Nikhil Oza Intern BvdumcMaheboob GanjalNo ratings yet
- 10 Approved Herbal Plants by DOHDocument7 pages10 Approved Herbal Plants by DOHjhommmmm88% (42)
- TUBERCULOSISDocument47 pagesTUBERCULOSISIfeoluwa Deborah Olopade100% (1)
- Practice Bulletin Multifetal GestationDocument16 pagesPractice Bulletin Multifetal GestationSusana Torres0% (1)
- TuberculosisDocument28 pagesTuberculosisbuddysmbdNo ratings yet
- Infectious Diseases (1&2) : TuberculosisDocument67 pagesInfectious Diseases (1&2) : TuberculosisYesi SaputriNo ratings yet
- 10 - Infectious Diseases (9700 AS Biology)Document33 pages10 - Infectious Diseases (9700 AS Biology)ho100% (1)
- Blood Transfusion Protocols in NeonatesDocument12 pagesBlood Transfusion Protocols in NeonatesSupriya M A SuppiNo ratings yet
- Case Study Pulmonary TuberculosisDocument19 pagesCase Study Pulmonary TuberculosisJester GalayNo ratings yet
- Trauma Ginjal: Sub Bagian Urologi Bagian/Smf Bedah FK Uns/Rsud Dr. MoewardiDocument39 pagesTrauma Ginjal: Sub Bagian Urologi Bagian/Smf Bedah FK Uns/Rsud Dr. MoewardiAtika SugiartoNo ratings yet
- Milking Procedure Pro PDFDocument2 pagesMilking Procedure Pro PDFIznulHaq ChughtaiNo ratings yet
- Diptheria Nursing ManagementDocument14 pagesDiptheria Nursing ManagementMey MeyNo ratings yet
- Diseases of Nervous SystemDocument30 pagesDiseases of Nervous SystemBangtan SonyeondanNo ratings yet
- Chapter 4: Comprehensive Geriatric Assessment: Multiple ChoiceDocument3 pagesChapter 4: Comprehensive Geriatric Assessment: Multiple ChoiceJamie100% (2)
- 3 - Pediatric TBDocument49 pages3 - Pediatric TBBirtukanNo ratings yet
- Tuberculosis (Mycobacterium Tuberculosis)Document106 pagesTuberculosis (Mycobacterium Tuberculosis)Gudeta shegerNo ratings yet
- 8.TB (Childhood TB)Document137 pages8.TB (Childhood TB)auNo ratings yet
- Influeza and Diptheria - DR Krishna Smirthi CVDocument28 pagesInflueza and Diptheria - DR Krishna Smirthi CVDr. Krishna SmirthiNo ratings yet
- Tuberculosis Unit 1 Lecture - 1Document39 pagesTuberculosis Unit 1 Lecture - 1Kubra Rasool100% (1)
- Jurnal - Fisiologi Kulit NeonatusDocument36 pagesJurnal - Fisiologi Kulit NeonatusMudrikahHaniyahNo ratings yet
- Cutaneous T.BDocument60 pagesCutaneous T.BSajin AlexanderNo ratings yet
- Hidalgo, Rubenjie S. Dela Cruz, Anthony Jericho B. Abary, Claudine D. Tan Hoc, Anne Mei H. Oca, Renx MarkDocument52 pagesHidalgo, Rubenjie S. Dela Cruz, Anthony Jericho B. Abary, Claudine D. Tan Hoc, Anne Mei H. Oca, Renx MarkEira LopezNo ratings yet
- Chapter 1-3Document18 pagesChapter 1-3Runi ArumndariNo ratings yet
- Pulmonary Tuberculosis: Survive Inside The MacrophagesDocument6 pagesPulmonary Tuberculosis: Survive Inside The MacrophagesDIVEN SolvonNo ratings yet
- HealthcareLec5 1Document5 pagesHealthcareLec5 1JAY JR. APONNo ratings yet
- Public Health 7Document5 pagesPublic Health 7Weird BoiNo ratings yet
- Mycobacterium Tuberculosis: Bañagado, Noreen B. Bs - Medical Technology 2Document4 pagesMycobacterium Tuberculosis: Bañagado, Noreen B. Bs - Medical Technology 2Noreen Bañagado100% (1)
- Pulmonary Tuberculosis, With Leprosy and HIV-Tuberculosis CoinfectionDocument74 pagesPulmonary Tuberculosis, With Leprosy and HIV-Tuberculosis CoinfectionMarc Imhotep Cray, M.D.No ratings yet
- Benito K. Lim Hong III, M.DDocument55 pagesBenito K. Lim Hong III, M.DCoy NuñezNo ratings yet
- Types of TuberculosisDocument7 pagesTypes of TuberculosisYashaswi ANo ratings yet
- Concept: Infection Exemplar: TuberculosisDocument6 pagesConcept: Infection Exemplar: Tuberculosisdlware3No ratings yet
- 4f. MycobacteriaDocument14 pages4f. MycobacteriaNOEMI BARROGANo ratings yet
- Clinical Manifestation of Oral TuberculosisDocument6 pagesClinical Manifestation of Oral TuberculosisSasa AprilaNo ratings yet
- Tuberculosis in ChildrenDocument96 pagesTuberculosis in Childrenped med0% (1)
- Case Series Primary Oral TBDocument7 pagesCase Series Primary Oral TBAnggy Natya ListyaningrumNo ratings yet
- Diphtheri 1Document22 pagesDiphtheri 1sakuraleeshaoranNo ratings yet
- Tuberculosis: Kristine SuguitanDocument10 pagesTuberculosis: Kristine SuguitanKish SuguitanNo ratings yet
- Airborne Transmission: Nurul Aqmar Mohd Nor Hazalin Phc454 - Pharmaceutical MicrobiologyDocument27 pagesAirborne Transmission: Nurul Aqmar Mohd Nor Hazalin Phc454 - Pharmaceutical MicrobiologySuhaila Abdul RahimNo ratings yet
- Bronchiolitis: Maud Meates-DennisDocument6 pagesBronchiolitis: Maud Meates-DennisMASIEL AMELIA BARRANTES ARCENo ratings yet
- TuberculosisDocument35 pagesTuberculosisAmr KhayyalNo ratings yet
- Tuberculosis: Mycobacterium Tuberculosis: 1. What Is M.tuberculosis?Document3 pagesTuberculosis: Mycobacterium Tuberculosis: 1. What Is M.tuberculosis?Quan ThieuNo ratings yet
- Cory Ne BacteriumDocument25 pagesCory Ne BacteriumjmalavanuNo ratings yet
- Tuberculosis (TB) and Anti TB Drugs: Dr. Haji Bahadar Pharmd, PHD Assistant Professor Kmu-IpmsDocument26 pagesTuberculosis (TB) and Anti TB Drugs: Dr. Haji Bahadar Pharmd, PHD Assistant Professor Kmu-IpmsHaniya KhanNo ratings yet
- W9 Measles German Measles Influenza Chicken Pox Covid19Document16 pagesW9 Measles German Measles Influenza Chicken Pox Covid19Jamie De LunaNo ratings yet
- Msir Jawaid Mmedical: MicrobiologyDocument28 pagesMsir Jawaid Mmedical: Microbiologykashif89No ratings yet
- Diphtheria and MeaslesDocument35 pagesDiphtheria and MeaslesMurugesanNo ratings yet
- TuberculosisDocument76 pagesTuberculosissashmita rautNo ratings yet
- Topic 31. TuberculosisDocument6 pagesTopic 31. TuberculosisAdeleye John AdebolaNo ratings yet
- Antimycobacterials and AntiviralsDocument65 pagesAntimycobacterials and AntiviralsAndile MoloiNo ratings yet
- Pneumonia in Under-5 ChildrenDocument34 pagesPneumonia in Under-5 Childrenmarte robiul saniNo ratings yet
- ScienceDocument23 pagesScienceTEE HAN LIN MoeNo ratings yet
- MycobacteriumDocument9 pagesMycobacteriumمحمد رائد رزاق إسماعيلNo ratings yet
- Applications of Biotechnology in Medicine SendingDocument30 pagesApplications of Biotechnology in Medicine SendingHaruka NanakiNo ratings yet
- Pulmonary TuberculosisDocument6 pagesPulmonary TuberculosisVanessa MolinaNo ratings yet
- Communicable Diseasesp.170 199Document30 pagesCommunicable Diseasesp.170 199Gary Largosa GallardoNo ratings yet
- Tuberculosis: College of NursingDocument9 pagesTuberculosis: College of NursingJoi Owen Yap TevesNo ratings yet
- Communicable Diseases - ReportDocument8 pagesCommunicable Diseases - ReportSheena Marie M. TarleNo ratings yet
- Bio Project RDocument20 pagesBio Project RSanjukth100% (1)
- Urinary Tract InfectionDocument20 pagesUrinary Tract InfectionFaraz SiddiquiNo ratings yet
- Immunology: MicrobiologyDocument7 pagesImmunology: MicrobiologyRemus MarasiganNo ratings yet
- Open Infections 2Document76 pagesOpen Infections 2Jehad AlzubairNo ratings yet
- East Africa University Bosaso, Puntland Somalia Faculty of Medicine Communicable Disease MR Buruj Ali SaladDocument42 pagesEast Africa University Bosaso, Puntland Somalia Faculty of Medicine Communicable Disease MR Buruj Ali SaladShaimaa AbdulkadirNo ratings yet
- Effects of Food Habits On Menstrual Cycle Among Adolescent GirlsDocument10 pagesEffects of Food Habits On Menstrual Cycle Among Adolescent GirlsDon Baraka DanielNo ratings yet
- Day 1 - GynacologyDocument204 pagesDay 1 - GynacologyTingting GeNo ratings yet
- LAS HEALTH 6 Q4 Wk5 Cherlyn. RonquilloDocument4 pagesLAS HEALTH 6 Q4 Wk5 Cherlyn. RonquilloANGELINA RAMBOYONGNo ratings yet
- Virome Characterization and Identification of A Putative Parvovirus and Poxvirus in Bat Ectoparasites of Yunnan ProvinceDocument38 pagesVirome Characterization and Identification of A Putative Parvovirus and Poxvirus in Bat Ectoparasites of Yunnan ProvinceemilioNo ratings yet
- 1998 Does Knuckle Cracking Lead To Arthritis of The Fingers PDFDocument2 pages1998 Does Knuckle Cracking Lead To Arthritis of The Fingers PDFMatías RamírezNo ratings yet
- Lithotripsy Salivary Stones OhpDocument5 pagesLithotripsy Salivary Stones Ohpaysha mksNo ratings yet
- Assessment Nursing Diagnosis Objective of Care Intervention RationaleDocument2 pagesAssessment Nursing Diagnosis Objective of Care Intervention Rationaleahmad ryanNo ratings yet
- US BTC FAQ 2015 Updated 1-5-16Document21 pagesUS BTC FAQ 2015 Updated 1-5-16Seau Vin NeeNo ratings yet
- Outscraper 2024020607591330fd Obstetrician Gynecologist +3Document265 pagesOutscraper 2024020607591330fd Obstetrician Gynecologist +3sanjulata.agriNo ratings yet
- Early Orthodontic Treatment of Skeletal Open-Bite MalocclusionDocument7 pagesEarly Orthodontic Treatment of Skeletal Open-Bite MalocclusionMaria SilvaNo ratings yet
- 2019 2020 Health History ExamDocument2 pages2019 2020 Health History Examsaranya purushothamanNo ratings yet
- Dietary Supplements in Dermatology: A Review of The Evidence For Zinc, Biotin, Vitamin D, Nicotinamide, and PolypodiumDocument9 pagesDietary Supplements in Dermatology: A Review of The Evidence For Zinc, Biotin, Vitamin D, Nicotinamide, and PolypodiumNazihan Safitri AlkatiriNo ratings yet
- Mechanism Readmisi Referral Pattern Degenerative Diseases With The Claim of Bpjs in In-Patient Departement Rsud DR.H Soewondo Kendal The Year 2015Document8 pagesMechanism Readmisi Referral Pattern Degenerative Diseases With The Claim of Bpjs in In-Patient Departement Rsud DR.H Soewondo Kendal The Year 2015ᎷᏒ.ᏴᎬᎪᏚᎢ.No ratings yet
- Hospital Diet and Oral Nutritional Supplements (Sip Feeds)Document16 pagesHospital Diet and Oral Nutritional Supplements (Sip Feeds)Patrick nyawiraNo ratings yet
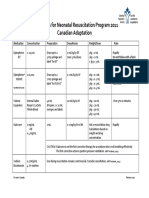
- Medications For Neonatal Resuscitation Program 2011 Canadian AdaptationDocument1 pageMedications For Neonatal Resuscitation Program 2011 Canadian AdaptationrubymayNo ratings yet
- LBM 6 Blok 20 SGD 1Document8 pagesLBM 6 Blok 20 SGD 1Ani LabibahNo ratings yet
- 5 Sore ThroatDocument45 pages5 Sore ThroatNurul Wandasari SNo ratings yet
- A 5-Year Observation of The Dahl Principle To Manage Localized Anterior Tooth WearDocument5 pagesA 5-Year Observation of The Dahl Principle To Manage Localized Anterior Tooth WearMohammad Abdulmon’emNo ratings yet
- 3 - Harada Mori TechniqueDocument2 pages3 - Harada Mori TechniqueHONEYLYNNE DELA TORRENo ratings yet
- Jadwal Pit (Uroginekologi Room)Document3 pagesJadwal Pit (Uroginekologi Room)Dwi Adi NugrohoNo ratings yet
- ADV 11-12-15.9-FinalDocument1 pageADV 11-12-15.9-FinalWilliam Floyd School DistrictNo ratings yet
- CD39 A Promising Target in Oncology PDFDocument9 pagesCD39 A Promising Target in Oncology PDFGeorge Sebastian AntonyNo ratings yet