You might also like
- Manage Animal Bites & Prevent RabiesDocument10 pagesManage Animal Bites & Prevent RabiesWilly WizeNo ratings yet
- National Rabies Control Programme GuidelineDocument7 pagesNational Rabies Control Programme GuidelineHari Pawan Kishore GarimellaNo ratings yet
- RabiesDocument32 pagesRabiesKareen Mae Porras BieneNo ratings yet
- Category Type of Exposure ManagementDocument10 pagesCategory Type of Exposure ManagementDianne GalangNo ratings yet
- Updated Guidelines on Management of Animal Bite PatientsDocument15 pagesUpdated Guidelines on Management of Animal Bite PatientsKaren ArchesNo ratings yet
- DOH SBIRT ClientflowDocument54 pagesDOH SBIRT ClientflowErin SantosNo ratings yet
- 10 Doh Programs: Prepared By: Dhonnalyn A. Caballero, RNDocument28 pages10 Doh Programs: Prepared By: Dhonnalyn A. Caballero, RNAnne Geleen BariasNo ratings yet
- IMCI Handouts BY: Claudette S. AdvinculaDocument7 pagesIMCI Handouts BY: Claudette S. AdvinculaRosemary Joy SiarotNo ratings yet
- National TB ControlDocument25 pagesNational TB Controlnirmal2444No ratings yet
- ESR Verification Form ReviseDocument4 pagesESR Verification Form ReviseRouella DoverteNo ratings yet
- 1.0 Functionality of The Local Health BoardDocument3 pages1.0 Functionality of The Local Health BoardEivenn Panerio100% (2)
- TB PolicyDocument33 pagesTB Policyyam kuan100% (1)
- TuberculosisDocument6 pagesTuberculosisZechariah NicholasNo ratings yet
- Record pneumococcal vaccinationDocument1 pageRecord pneumococcal vaccinationalfredtan6288No ratings yet
- R.A. 9482Document4 pagesR.A. 9482KatNo ratings yet
- Handouts Comminicable Disease by DR SalvadorDocument24 pagesHandouts Comminicable Disease by DR SalvadorrachaelNo ratings yet
- DTTB Hiring DeploymentDocument2 pagesDTTB Hiring DeploymentIsrael GoticoNo ratings yet
- dm2020 0439 Omnibus Guidelines PDITR PDFDocument44 pagesdm2020 0439 Omnibus Guidelines PDITR PDFCathryn OrlandaNo ratings yet
- Hypertension and Diabetes ClubDocument15 pagesHypertension and Diabetes Clubncd.bulacanNo ratings yet
- PhilHealth Konsulta Provider Self-Assessment ToolDocument8 pagesPhilHealth Konsulta Provider Self-Assessment ToolFret Ramirez Coronia RNNo ratings yet
- Activity Design June 2017 Program Title: Iclinicsys Training RationaleDocument2 pagesActivity Design June 2017 Program Title: Iclinicsys Training Rationalepedrong dodongNo ratings yet
- 1 - Overview Training of The Revised MOP 6th Ed.Document14 pages1 - Overview Training of The Revised MOP 6th Ed.RHU Minalabac100% (1)
- FHSISDocument14 pagesFHSISSam Raven AndresNo ratings yet
- Annex A - Self-Assessment Tool For Proposed EPCB Health Facilities PDFDocument5 pagesAnnex A - Self-Assessment Tool For Proposed EPCB Health Facilities PDFCora Mendoza100% (1)
- Expanded Immunization PorgramDocument6 pagesExpanded Immunization PorgramJavie Bryant RedilNo ratings yet
- Policies-Tb Dots in The WorkplaceDocument5 pagesPolicies-Tb Dots in The WorkplaceAngelique ThomasNo ratings yet
- TCL For Nutrition & Epi Program Part 1Document23 pagesTCL For Nutrition & Epi Program Part 1Johnmark DubdubanNo ratings yet
- Administrative Deployment in Region XIDocument3 pagesAdministrative Deployment in Region XIMuhammad IbrahimNo ratings yet
- Letter of Intent For Health FacilityDocument1 pageLetter of Intent For Health FacilityTianDy OirasNo ratings yet
- NiE Plan - 2021finalDocument24 pagesNiE Plan - 2021finaljonahNo ratings yet
- MANAGING DOG/CAT BITES AT HEALTH FACILITYDocument5 pagesMANAGING DOG/CAT BITES AT HEALTH FACILITYleo89azman100% (1)
- Infection: BascisDocument66 pagesInfection: Bascistummalapalli venkateswara raoNo ratings yet
- Management of MDR-TBDocument270 pagesManagement of MDR-TBLukman HidayatNo ratings yet
- Labour RecordDocument3 pagesLabour RecordmerryNo ratings yet
- VaccinationDocument28 pagesVaccinationM AQIB ASLAMNo ratings yet
- National Objectives For HealthDocument85 pagesNational Objectives For HealthJesserene SorianoNo ratings yet
- F1 Plus Botika NG Bayan Manual of ProceduresDocument33 pagesF1 Plus Botika NG Bayan Manual of ProceduresArdenNo ratings yet
- Arcadio - Newborn ScreeningDocument63 pagesArcadio - Newborn ScreeningkoalaNo ratings yet
- NCD National PolicyDocument14 pagesNCD National PolicyHerlene Lyneth ZalamedaNo ratings yet
- PHC2. The Philippine Health Care Delivery SystemDocument55 pagesPHC2. The Philippine Health Care Delivery SystemHumilyn NgayawonNo ratings yet
- CHN TopicsDocument19 pagesCHN TopicsKristine AnaenNo ratings yet
- NCM 119 Assignment Galutan Kimberly Erika FDocument5 pagesNCM 119 Assignment Galutan Kimberly Erika Faaron tabernaNo ratings yet
- Gad Annual Plan and BudgetDocument2 pagesGad Annual Plan and BudgetRaquel dg.BulaongNo ratings yet
- IMCI Session 3-The Integrated Case Management ProcessDocument67 pagesIMCI Session 3-The Integrated Case Management Processsarguss1480% (5)
- MCN TransDocument8 pagesMCN TransHecia Marie Gaga-aNo ratings yet
- RA 7305 (Magna Carta For Health Workers) PDFDocument57 pagesRA 7305 (Magna Carta For Health Workers) PDFBeboy Paylangco Evardo100% (1)
- Sanitary PermitDocument1 pageSanitary PermitImee CorreaNo ratings yet
- Animal Bite Traetment CenterDocument5 pagesAnimal Bite Traetment CenterPaul Cenabre100% (1)
- DEMOGRAPHIC INDICATORSDocument3 pagesDEMOGRAPHIC INDICATORSAdiel Calsa100% (1)
- Preparation of Microplan of Routine Immunization and Consolidation at Block-District LevelDocument9 pagesPreparation of Microplan of Routine Immunization and Consolidation at Block-District LevelNational Child Health Resource Centre (NCHRC)No ratings yet
- Ibajay District Hospital Frontline Services GuidePERIOD TOCOVERPERSON TOAPPROACH1 minuteLaboratory Aide5 minutesLaboratory Aide5 minutesCashier10 minutesLab TechnicianDocument22 pagesIbajay District Hospital Frontline Services GuidePERIOD TOCOVERPERSON TOAPPROACH1 minuteLaboratory Aide5 minutesLaboratory Aide5 minutesCashier10 minutesLab TechnicianMary Jean GelitoNo ratings yet
- Referral PhilippinesDocument42 pagesReferral Philippinesemed vsmmcNo ratings yet
- Public Health Program Family HealthDocument183 pagesPublic Health Program Family HealthPrince Jhessie L. Abella100% (1)
- Magna CartaDocument56 pagesMagna CartaJastine Beltran - PerezNo ratings yet
- What Is Rabies? How Do People and Animals Get The Disease?Document14 pagesWhat Is Rabies? How Do People and Animals Get The Disease?lea nicole iglesiasNo ratings yet
- Assignment (2) : The Republic of Iraq Ministry of Higher Education and Scientific ResearchDocument6 pagesAssignment (2) : The Republic of Iraq Ministry of Higher Education and Scientific ResearchBright StarNo ratings yet
- Situational Analysis EPI 2015 Final 1Document9 pagesSituational Analysis EPI 2015 Final 1At Day's Ward0% (1)
- Guideline for Prevention and Control of Rabies in MalaysiaDocument17 pagesGuideline for Prevention and Control of Rabies in MalaysiavcweeNo ratings yet
- Rabies ContentDocument3 pagesRabies ContentKim AquinoNo ratings yet
- Rabies Policies and ProceduresDocument19 pagesRabies Policies and ProceduresFret Ramirez Coronia RNNo ratings yet
- Aztecs and IncasDocument14 pagesAztecs and Incasjamesryan831No ratings yet
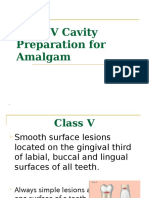
- Class VDocument37 pagesClass VyahyaNo ratings yet
- Food ListDocument1 pageFood ListScott PalmerNo ratings yet
- Diversity of BacteriaDocument3 pagesDiversity of BacteriaLisa AllisyaNo ratings yet
- Biological Classification Class 11 Notes Biology CDocument14 pagesBiological Classification Class 11 Notes Biology Cdharun0704No ratings yet
- Ringkasan Dari Icd - Gemala Hatta (2012)Document5 pagesRingkasan Dari Icd - Gemala Hatta (2012)zenalNo ratings yet
- Pediatrics QuestionsDocument22 pagesPediatrics QuestionsShaik AmreenNo ratings yet
- Bacteriology - Semifinals - Neisseria and MoraxellaDocument10 pagesBacteriology - Semifinals - Neisseria and MoraxellaUshuaia Ira Marie L. GallaronNo ratings yet
- The Role of Nurses in Providing Sex Education for HIV/AIDS PatientsDocument15 pagesThe Role of Nurses in Providing Sex Education for HIV/AIDS PatientsXHavierNo ratings yet
- Week 8 - Bacteriology LectureDocument7 pagesWeek 8 - Bacteriology LectureReangg SerranoNo ratings yet
- Eleanor McBean & Trung Nguyen - The Poisoned Needle: Suppressed Facts About Vaccination (2018 Update)Document337 pagesEleanor McBean & Trung Nguyen - The Poisoned Needle: Suppressed Facts About Vaccination (2018 Update)Adna100% (2)
- Weilfelixtest 120213194736 Phpapp02Document19 pagesWeilfelixtest 120213194736 Phpapp02nitish-bhardwaj-9810No ratings yet
- PRINCIPLES OF DISEASE PREVENTIONDocument13 pagesPRINCIPLES OF DISEASE PREVENTIONAYO NELSON0% (1)
- CFR - Why Vaccination Coverage Is Crucial for COVID-19Document9 pagesCFR - Why Vaccination Coverage Is Crucial for COVID-19ioannis tsagarliotisNo ratings yet
- Turtles All The Way Down: Vaccine Science and MythDocument275 pagesTurtles All The Way Down: Vaccine Science and MythCristina CidadeNo ratings yet
- EID JournalDocument175 pagesEID JournalArthur Boegaurd100% (1)
- Dr. Jane P. Messina, March 2014Document5 pagesDr. Jane P. Messina, March 2014Janey MessinaNo ratings yet
- Public Health COC ExamDocument19 pagesPublic Health COC ExamTut Kong RuachNo ratings yet
- Para LabDocument22 pagesPara LabClaudine DelacruzNo ratings yet
- Hot Topics in Internal MedicineDocument9 pagesHot Topics in Internal Medicinekhangsiean89No ratings yet
- Infection Control Practices in Healthcare SettingDocument89 pagesInfection Control Practices in Healthcare SettingArvic Pascua MaltizoNo ratings yet
- Revision Study Material Unit - X: Anti-Viral & HIV DrugsDocument16 pagesRevision Study Material Unit - X: Anti-Viral & HIV DrugsMagesh SNo ratings yet
- 2011 Veterinary Vaccinesand Their Importanceto Animal Healthand Public HealthDocument11 pages2011 Veterinary Vaccinesand Their Importanceto Animal Healthand Public HealthCARLOTA DIAZ AGUILARNo ratings yet
- Is My Stethoscope Harmless?: Operating Room Stethoscopes Under MicroscopesDocument9 pagesIs My Stethoscope Harmless?: Operating Room Stethoscopes Under MicroscopesIJAR JOURNALNo ratings yet
- Acute Respiratory Tract Infections in ChildrenDocument31 pagesAcute Respiratory Tract Infections in ChildrenNaushad AlamNo ratings yet
- BIO104E Microbiology and Parasitology Multiple Choice QuestionsDocument3 pagesBIO104E Microbiology and Parasitology Multiple Choice QuestionsStephen AzaresNo ratings yet
- Laundry Infection Control ChecklistDocument2 pagesLaundry Infection Control ChecklistSea Gate100% (1)
- Bio ManualDocument4 pagesBio ManualshreyaNo ratings yet
- Mass Gathering ManagementDocument85 pagesMass Gathering ManagementAmalkrishnaNo ratings yet