You might also like
- Animal Bite Module 2021Document20 pagesAnimal Bite Module 2021ERMED OFC R2TMCNo ratings yet
- Animal Bite Traetment CenterDocument5 pagesAnimal Bite Traetment CenterPaul Cenabre100% (1)
- Rhu Citizen CharterDocument18 pagesRhu Citizen CharteradrianNo ratings yet
- Reporting of Diseases and Health Events OrdinanceDocument10 pagesReporting of Diseases and Health Events OrdinanceRacquel FrondaNo ratings yet
- Manual On The PEN Protocol On The Integrated Management of Hypertension and DiabetesDocument61 pagesManual On The PEN Protocol On The Integrated Management of Hypertension and DiabetesRanda Noray100% (2)
- dm2020 0439 Omnibus Guidelines PDITR PDFDocument44 pagesdm2020 0439 Omnibus Guidelines PDITR PDFCathryn OrlandaNo ratings yet
- AOP-2024-narrative FINALDocument66 pagesAOP-2024-narrative FINALjasper manuelNo ratings yet
- FINAL-Guinayangan AOP 2024Document46 pagesFINAL-Guinayangan AOP 2024Myrna OrnedoNo ratings yet
- Policies and Procedure For Ensuring Quality of Sputum Microscopy ResultsDocument2 pagesPolicies and Procedure For Ensuring Quality of Sputum Microscopy ResultsReinald Raven GuerreroNo ratings yet
- ABTC Assessment ToolDocument8 pagesABTC Assessment Toolyam kuanNo ratings yet
- DM No. 2023 0083 Guidelines For The FHSIS Data Validation and Reconciliation - 22feb2023 2Document11 pagesDM No. 2023 0083 Guidelines For The FHSIS Data Validation and Reconciliation - 22feb2023 2Carlen Mae L. YacapinNo ratings yet
- DRRM H 2020 ScribdDocument186 pagesDRRM H 2020 ScribdTagubilin JuliusNo ratings yet
- The DRRM-H System: (Achieved/ On-Going/ Not Yet Started)Document3 pagesThe DRRM-H System: (Achieved/ On-Going/ Not Yet Started)maria_abigailNo ratings yet
- AO 101, s.2003. National Policy On Oral HealthDocument7 pagesAO 101, s.2003. National Policy On Oral HealthJosephine FawayanNo ratings yet
- AOP OPD Finalsituational and GAP AnalysisDocument2 pagesAOP OPD Finalsituational and GAP AnalysisJennylyn GuadalupeNo ratings yet
- Iloilo City Regulation Ordinance 2015-029Document4 pagesIloilo City Regulation Ordinance 2015-029Iloilo City Council100% (1)
- Universal Health Care Act Provides Comprehensive CoverageDocument17 pagesUniversal Health Care Act Provides Comprehensive CoverageJude Avorque Acidre100% (1)
- Baliangao DRRM-H 2023-2025 As of Oct 23, 2023 UpdatedDocument92 pagesBaliangao DRRM-H 2023-2025 As of Oct 23, 2023 UpdatedRoel AbricaNo ratings yet
- Self Assessment FormDocument15 pagesSelf Assessment FormRitchie Rich Pangilinan Villareal63% (8)
- Dokument - Pub DRRM H Planning Guide Module 2 Flipbook PDFDocument10 pagesDokument - Pub DRRM H Planning Guide Module 2 Flipbook PDFMohrein H. Ismael VI100% (1)
- DOH HEMS Guidelines on Hospital Alert SystemsDocument6 pagesDOH HEMS Guidelines on Hospital Alert SystemsIna RamosNo ratings yet
- The Health Promotion HandbookDocument63 pagesThe Health Promotion HandbookOnyd Subingsubing100% (1)
- QPMC Liph 2019Document69 pagesQPMC Liph 2019JovelleAnneMondragonNo ratings yet
- MNC Res 7. EO 51Document3 pagesMNC Res 7. EO 51ann29No ratings yet
- DRRM-H Advocacy KitDocument32 pagesDRRM-H Advocacy KitERMED OFC R2TMC100% (1)
- Position and Competency Profile: Job SummaryDocument8 pagesPosition and Competency Profile: Job SummaryGiovani CalivaNo ratings yet
- Abra DRRMH EoDocument3 pagesAbra DRRMH EoPidigan RHUNo ratings yet
- MNDRS Manual of OperationsDocument34 pagesMNDRS Manual of OperationsPHO AntNo ratings yet
- NIP Data Reporting, Data Quality Check and AnalysisDocument185 pagesNIP Data Reporting, Data Quality Check and AnalysisbonNo ratings yet
- Animal Bite FlowchartDocument1 pageAnimal Bite FlowchartBdh AbtcNo ratings yet
- Barangay Health Workers' Benefits and Incentives OrdinanceDocument8 pagesBarangay Health Workers' Benefits and Incentives Ordinancebash bash100% (1)
- Annual Operational Plan 2012 NarrativeDocument11 pagesAnnual Operational Plan 2012 NarrativeArianne A ZamoraNo ratings yet
- Philippine Integrated Management of Acute Malnnutrition PDFDocument53 pagesPhilippine Integrated Management of Acute Malnnutrition PDFTherese SyNo ratings yet
- Draft Ordinance (Birthing Homes Regulation)Document8 pagesDraft Ordinance (Birthing Homes Regulation)Zimm BasubasNo ratings yet
- R A 10152Document3 pagesR A 10152Cesar Valera100% (3)
- FINAL-Guinayangan AOP 2024Document39 pagesFINAL-Guinayangan AOP 2024Myrna Ornedo100% (1)
- UHC PresentationDocument21 pagesUHC PresentationHarold Paulo Mejia100% (1)
- Philippines Health Emergency Assessment ReportDocument1 pagePhilippines Health Emergency Assessment ReportDELIVERY ROOMNo ratings yet
- HEARS REPORT FormDocument1 pageHEARS REPORT FormBarangay Guinayang San MateoNo ratings yet
- HCPNDocument27 pagesHCPNJohn Philip TiongcoNo ratings yet
- Afhf Level 2Document3 pagesAfhf Level 2ela bachii100% (1)
- Self-Assessment Form Official-ABTCDocument28 pagesSelf-Assessment Form Official-ABTCJanice Villaroya Jarales-YusonNo ratings yet
- HESU OrganogramDocument29 pagesHESU OrganogramHEMS SAMCH100% (4)
- MHO Operations ManualDocument33 pagesMHO Operations ManualHarnikka ConstantinoNo ratings yet
- DohDocument103 pagesDohRapSamputonNo ratings yet
- FINAL-Guinayangan AOP 2024Document33 pagesFINAL-Guinayangan AOP 2024Myrna Ornedo100% (2)
- Activity Plan: Barangay LapuDocument5 pagesActivity Plan: Barangay LapuInchic Miranda0% (1)
- Pidsr CifDocument17 pagesPidsr CifAbraham Asto100% (4)
- Target Client List For Nutrition and Expanded Program For ImmunizationDocument7 pagesTarget Client List For Nutrition and Expanded Program For ImmunizationEden Vblagasy0% (1)
- Ao2023 0009 PDFDocument54 pagesAo2023 0009 PDFJohn Philip TiongcoNo ratings yet
- Abtc-Self-Assessment - 2023Document8 pagesAbtc-Self-Assessment - 2023yam kuanNo ratings yet
- DOH SBIRT ClientflowDocument54 pagesDOH SBIRT ClientflowErin SantosNo ratings yet
- The PhilCAT Certification Self-Assessment and Survey Tool (Repaired) FinALDocument25 pagesThe PhilCAT Certification Self-Assessment and Survey Tool (Repaired) FinALMark Johnuel Duavis93% (14)
- BHB Orientation For NDPs-1Document19 pagesBHB Orientation For NDPs-1Shevan Simon AliñabonNo ratings yet
- Vaccines, Cold Chain and Logistics Management: Manual of OperationsDocument148 pagesVaccines, Cold Chain and Logistics Management: Manual of Operationscesspintas Cuaresma67% (3)
- ADEPTDocument11 pagesADEPTAthosLouisEscalante100% (1)
- Office of The SecretaryDocument11 pagesOffice of The SecretaryAdrian Doctolero100% (5)
- LGU Scorecard DC 2022-0273Document96 pagesLGU Scorecard DC 2022-0273Jomelle WongNo ratings yet
- Rabies & Snake BiteDocument32 pagesRabies & Snake BiteJoy BogadorNo ratings yet
- Animal Bite: Pablo R. Quedado, MDDocument36 pagesAnimal Bite: Pablo R. Quedado, MDPrincess Noreen SavellanoNo ratings yet
- Network and IT Assessment Form 1Document1 pageNetwork and IT Assessment Form 1Fret Ramirez Coronia RNNo ratings yet
- PhilHealth Konsulta Provider Self-Assessment ToolDocument8 pagesPhilHealth Konsulta Provider Self-Assessment ToolFret Ramirez Coronia RNNo ratings yet
- Chikiting Ligtas Certificate TemplateDocument2 pagesChikiting Ligtas Certificate TemplateRhu Pugo, La UnionNo ratings yet
- DRRMH Monitoring and Assessment ChecklistDocument3 pagesDRRMH Monitoring and Assessment ChecklistFret Ramirez Coronia RNNo ratings yet
- Network and IT Assessment Form 2Document1 pageNetwork and IT Assessment Form 2Fret Ramirez Coronia RNNo ratings yet
- Advisory No. 15Document9 pagesAdvisory No. 15Fret Ramirez Coronia RNNo ratings yet
- Republic The Philippines Health: ClarifyDocument12 pagesRepublic The Philippines Health: ClarifyFret Ramirez Coronia RNNo ratings yet
- Product Information of Sinopharm Covid-19 Vaccine (Vero Cell), Inactivated CoviloDocument7 pagesProduct Information of Sinopharm Covid-19 Vaccine (Vero Cell), Inactivated CoviloFret Ramirez Coronia RNNo ratings yet
- Network and IT Assessment Form 3Document1 pageNetwork and IT Assessment Form 3Fret Ramirez Coronia RNNo ratings yet
- Training Rules and Regulations: Rizal ChapterDocument1 pageTraining Rules and Regulations: Rizal ChapterFret Ramirez Coronia RNNo ratings yet
- Social Change1Document9 pagesSocial Change1Fret Ramirez Coronia RNNo ratings yet
- Dokument - Pub DRRM H Planning Guide Content Module 3 Flipbook PDFDocument9 pagesDokument - Pub DRRM H Planning Guide Content Module 3 Flipbook PDFFret Ramirez Coronia RNNo ratings yet
- AO2021-0043 Omnibus Guidelines On The Minimum Public Health Standards For The Safe Reopening of Institutions (08-31)Document44 pagesAO2021-0043 Omnibus Guidelines On The Minimum Public Health Standards For The Safe Reopening of Institutions (08-31)Fret Ramirez Coronia RN100% (1)
- DOH 2020-0258-A Amended GuidelinesDocument7 pagesDOH 2020-0258-A Amended GuidelinesCathy LopezNo ratings yet
- Index Case Name Age Sex Contact Generation Date of Birth (Mm/dd/yr)Document5 pagesIndex Case Name Age Sex Contact Generation Date of Birth (Mm/dd/yr)Fret Ramirez Coronia RNNo ratings yet
- Burns Management PDFDocument7 pagesBurns Management PDFRoh Bungaria N Garingging100% (1)
- Dialysis Flow SheetDocument1 pageDialysis Flow SheetFret Ramirez Coronia RNNo ratings yet
- National Vaccination Operation Center: COVID-19 VACCINE HAYAT-VAX (Sinopharm)Document9 pagesNational Vaccination Operation Center: COVID-19 VACCINE HAYAT-VAX (Sinopharm)Fret Ramirez Coronia RNNo ratings yet
- NVOC Advisory 41 Reiteration On The Scheduling For Vaccination of Individuals With COVID-19 InfectionDocument1 pageNVOC Advisory 41 Reiteration On The Scheduling For Vaccination of Individuals With COVID-19 InfectionFret Ramirez Coronia RNNo ratings yet
- Skill Mapping20210531 - 19132706Document4 pagesSkill Mapping20210531 - 19132706Fret Ramirez Coronia RNNo ratings yet
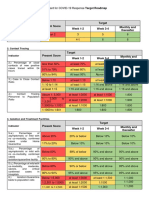
- Present Score Target Week 1-2 Week 3-4 Monthly and ThereafterDocument2 pagesPresent Score Target Week 1-2 Week 3-4 Monthly and ThereafterFret Ramirez Coronia RNNo ratings yet
- ANTIGEN TEST KIT UTILIZATION REPORT - Preliminary FormDocument1 pageANTIGEN TEST KIT UTILIZATION REPORT - Preliminary FormFret Ramirez Coronia RNNo ratings yet
- QAQI - Policy On QAPDocument5 pagesQAQI - Policy On QAPFret Ramirez Coronia RNNo ratings yet
- Guide During AEFI InvestigationDocument1 pageGuide During AEFI InvestigationFret Ramirez Coronia RNNo ratings yet
- LGU Specimen Submission GuidelinesDocument3 pagesLGU Specimen Submission GuidelinesFret Ramirez Coronia RNNo ratings yet
- Vital Signs Flow SheetDocument1 pageVital Signs Flow SheetFret Ramirez Coronia RNNo ratings yet
- Regulatory Board's Guide to Registering Housing ProjectsDocument16 pagesRegulatory Board's Guide to Registering Housing ProjectsLgu SikatunaNo ratings yet
- Medication LogDocument1 pageMedication LogFret Ramirez Coronia RNNo ratings yet
- Cstms Registry CalabarzonDocument11 pagesCstms Registry CalabarzonFret Ramirez Coronia RNNo ratings yet
- Hotel Training ReportDocument14 pagesHotel Training ReportButchick Concepcion Malasa100% (1)
- Ken Jennings' Junior Genius Guides: Maps and Geography (Excerpt)Document24 pagesKen Jennings' Junior Genius Guides: Maps and Geography (Excerpt)Simon and Schuster100% (2)
- COLORMATCHING GUIDELINES FOR DEMI-PERMANENT HAIR COLORDocument1 pageCOLORMATCHING GUIDELINES FOR DEMI-PERMANENT HAIR COLORss bbNo ratings yet
- BuildingDocument156 pagesBuildingMaya MayaNo ratings yet
- Social Responsibility and Managerial Ethics (Principles of Management)Document35 pagesSocial Responsibility and Managerial Ethics (Principles of Management)Reader94% (16)
- Drewry Capability StatementDocument9 pagesDrewry Capability Statementmanis_sgsNo ratings yet
- CẤU TẠO TỪ VÀ TỪ LOẠIDocument15 pagesCẤU TẠO TỪ VÀ TỪ LOẠIccnsdNo ratings yet
- Nanotechnology in TextilesDocument4 pagesNanotechnology in Textileskevin cagud PhillipNo ratings yet
- TR 101 - Issue 2Document101 pagesTR 101 - Issue 2ergismiloNo ratings yet
- Treatment: Animated Text Onstage:: Topic: Learning Objective: WMS Packages Module Introduction Display 1Document8 pagesTreatment: Animated Text Onstage:: Topic: Learning Objective: WMS Packages Module Introduction Display 1hikikNo ratings yet
- Business LetterDocument196 pagesBusiness LetterNulaNo ratings yet
- Cucs 016 13 PDFDocument16 pagesCucs 016 13 PDFAnonymous SlyvspdBNo ratings yet
- Rogers Lacaze Case InfoDocument1 pageRogers Lacaze Case InfomakeawishNo ratings yet
- Kindergarten Quarter 4 Standards For Lesson PlansDocument2 pagesKindergarten Quarter 4 Standards For Lesson PlansLydiaDietschNo ratings yet
- Lesson 1 G8Document11 pagesLesson 1 G8Malorie Dela CruzNo ratings yet
- Itm Guia Rapida Tds 600 Tipo4 Ed1 EspDocument148 pagesItm Guia Rapida Tds 600 Tipo4 Ed1 Espcamel2003No ratings yet
- Class9-NTSE MATH WORKSHEETDocument4 pagesClass9-NTSE MATH WORKSHEETJeetu RaoNo ratings yet
- Haven, Quantum Social ScienceDocument306 pagesHaven, Quantum Social ScienceMichael H. HejaziNo ratings yet
- Basics: Architectural Design Designing Architecture Language of Space and Form Diagramming The Big Idea and ArchitectureDocument7 pagesBasics: Architectural Design Designing Architecture Language of Space and Form Diagramming The Big Idea and ArchitectureNaveen KishoreNo ratings yet
- Dodigen 2808 TDSDocument1 pageDodigen 2808 TDSRashid SaleemNo ratings yet
- Court Documents - Purdue Pharma CaseDocument236 pagesCourt Documents - Purdue Pharma CaseHung LeNo ratings yet
- Section 5: Finite Volume Methods For The Navier Stokes EquationsDocument27 pagesSection 5: Finite Volume Methods For The Navier Stokes EquationsUmutcanNo ratings yet
- 2016 Annual Report - Printer-ReadyDocument35 pages2016 Annual Report - Printer-ReadyDonna BrodberNo ratings yet
- Sap GlossaryDocument324 pagesSap GlossaryNikos TataliasNo ratings yet
- Nitrogen CycleDocument15 pagesNitrogen CycleKenji AlbellarNo ratings yet
- Mac 2009Document60 pagesMac 2009Ridwan Pramudya100% (1)
- Toufik Hossain Project On ODE Using Fourier TransformDocument6 pagesToufik Hossain Project On ODE Using Fourier TransformToufik HossainNo ratings yet
- Phillips Petroleum Co. v. Mississippi, 484 U.S. 469 (1988)Document21 pagesPhillips Petroleum Co. v. Mississippi, 484 U.S. 469 (1988)Scribd Government DocsNo ratings yet
- Woody Plant Seed Manual - CompleteDocument1,241 pagesWoody Plant Seed Manual - CompleteJonas Sandell100% (1)
- Clay Brick Making Machine Mew CB 3000Document5 pagesClay Brick Making Machine Mew CB 3000Aakansh NigamNo ratings yet