You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Assessment of Adult ADHDDocument24 pagesAssessment of Adult ADHDPsydoc100% (4)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Gender & Mental HealthDocument25 pagesGender & Mental HealthMarcNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Clinical Practice Guideline For Schizophrenia and Incipient Psychotic DisorderDocument9 pagesClinical Practice Guideline For Schizophrenia and Incipient Psychotic DisorderFranco MascayanoNo ratings yet
- Brain Cancer (Tumors) : Jinu Janet Varghese Group: 4 Year: 5 Tbilisi State Medical UniversityDocument35 pagesBrain Cancer (Tumors) : Jinu Janet Varghese Group: 4 Year: 5 Tbilisi State Medical UniversityPPDSNeuroUnsri RSMHNo ratings yet
- Introduction To Nursing EthicsDocument23 pagesIntroduction To Nursing EthicsAzra Baloch67% (3)
- ERP Bridging Document Rev 00Document21 pagesERP Bridging Document Rev 00herisusantoNo ratings yet
- To Err Is Human A Case Study of Error Prevention in Process IsolationsDocument6 pagesTo Err Is Human A Case Study of Error Prevention in Process Isolationsairbuk doeingNo ratings yet
- Dialysis Flow SheetDocument1 pageDialysis Flow SheetFret Ramirez Coronia RNNo ratings yet
- Dokument - Pub DRRM H Planning Guide Content Module 3 Flipbook PDFDocument9 pagesDokument - Pub DRRM H Planning Guide Content Module 3 Flipbook PDFFret Ramirez Coronia RNNo ratings yet
- PhilHealth Konsulta Provider Self-Assessment ToolDocument8 pagesPhilHealth Konsulta Provider Self-Assessment ToolFret Ramirez Coronia RNNo ratings yet
- Rabies Policies and ProceduresDocument19 pagesRabies Policies and ProceduresFret Ramirez Coronia RNNo ratings yet
- Sosialisasi E-Report IKP RS Eksternal - 2021Document32 pagesSosialisasi E-Report IKP RS Eksternal - 2021Putri Arum PermatasariNo ratings yet
- Comm 1010 Informative Full-Sentence Speech Outline InstructionsDocument2 pagesComm 1010 Informative Full-Sentence Speech Outline Instructionsapi-270505782No ratings yet
- Network and IT Assessment Form 1Document1 pageNetwork and IT Assessment Form 1Fret Ramirez Coronia RNNo ratings yet
- DRRMH Monitoring and Assessment ChecklistDocument3 pagesDRRMH Monitoring and Assessment ChecklistFret Ramirez Coronia RNNo ratings yet
- Chikiting Ligtas Certificate TemplateDocument2 pagesChikiting Ligtas Certificate TemplateRhu Pugo, La UnionNo ratings yet
- Network and IT Assessment Form 3Document1 pageNetwork and IT Assessment Form 3Fret Ramirez Coronia RNNo ratings yet
- Network and IT Assessment Form 2Document1 pageNetwork and IT Assessment Form 2Fret Ramirez Coronia RNNo ratings yet
- Training Rules and Regulations: Rizal ChapterDocument1 pageTraining Rules and Regulations: Rizal ChapterFret Ramirez Coronia RNNo ratings yet
- Social Change1Document9 pagesSocial Change1Fret Ramirez Coronia RNNo ratings yet
- Republic The Philippines Health: ClarifyDocument12 pagesRepublic The Philippines Health: ClarifyFret Ramirez Coronia RNNo ratings yet
- National Vaccination Operation Center: COVID-19 VACCINE HAYAT-VAX (Sinopharm)Document9 pagesNational Vaccination Operation Center: COVID-19 VACCINE HAYAT-VAX (Sinopharm)Fret Ramirez Coronia RNNo ratings yet
- DOH 2020-0258-A Amended GuidelinesDocument7 pagesDOH 2020-0258-A Amended GuidelinesCathy LopezNo ratings yet
- Advisory No. 15Document9 pagesAdvisory No. 15Fret Ramirez Coronia RNNo ratings yet
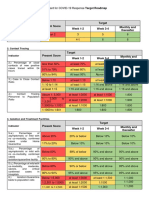
- Present Score Target Week 1-2 Week 3-4 Monthly and ThereafterDocument2 pagesPresent Score Target Week 1-2 Week 3-4 Monthly and ThereafterFret Ramirez Coronia RNNo ratings yet
- Product Information of Sinopharm Covid-19 Vaccine (Vero Cell), Inactivated CoviloDocument7 pagesProduct Information of Sinopharm Covid-19 Vaccine (Vero Cell), Inactivated CoviloFret Ramirez Coronia RNNo ratings yet
- AO2021-0043 Omnibus Guidelines On The Minimum Public Health Standards For The Safe Reopening of Institutions (08-31)Document44 pagesAO2021-0043 Omnibus Guidelines On The Minimum Public Health Standards For The Safe Reopening of Institutions (08-31)Fret Ramirez Coronia RN100% (1)
- Burns Management PDFDocument7 pagesBurns Management PDFRoh Bungaria N Garingging100% (1)
- Skill Mapping20210531 - 19132706Document4 pagesSkill Mapping20210531 - 19132706Fret Ramirez Coronia RNNo ratings yet
- Index Case Name Age Sex Contact Generation Date of Birth (Mm/dd/yr)Document5 pagesIndex Case Name Age Sex Contact Generation Date of Birth (Mm/dd/yr)Fret Ramirez Coronia RNNo ratings yet
- NVOC Advisory 41 Reiteration On The Scheduling For Vaccination of Individuals With COVID-19 InfectionDocument1 pageNVOC Advisory 41 Reiteration On The Scheduling For Vaccination of Individuals With COVID-19 InfectionFret Ramirez Coronia RNNo ratings yet
- QAQI - Policy On QAPDocument5 pagesQAQI - Policy On QAPFret Ramirez Coronia RNNo ratings yet
- Vital Signs Flow SheetDocument1 pageVital Signs Flow SheetFret Ramirez Coronia RNNo ratings yet
- ANTIGEN TEST KIT UTILIZATION REPORT - Preliminary FormDocument1 pageANTIGEN TEST KIT UTILIZATION REPORT - Preliminary FormFret Ramirez Coronia RNNo ratings yet
- Medication LogDocument1 pageMedication LogFret Ramirez Coronia RNNo ratings yet
- Regulatory Board's Guide to Registering Housing ProjectsDocument16 pagesRegulatory Board's Guide to Registering Housing ProjectsLgu SikatunaNo ratings yet
- LGU Specimen Submission GuidelinesDocument3 pagesLGU Specimen Submission GuidelinesFret Ramirez Coronia RNNo ratings yet
- Cstms Registry CalabarzonDocument11 pagesCstms Registry CalabarzonFret Ramirez Coronia RNNo ratings yet
- There and Back AgainDocument113 pagesThere and Back AgainsantjiejdNo ratings yet
- Cancer: Causes, Diagnosis & TreatmentDocument2 pagesCancer: Causes, Diagnosis & TreatmentNitesh kuraheNo ratings yet
- Case Study on ADHD Nursing Diagnoses and InterventionsDocument2 pagesCase Study on ADHD Nursing Diagnoses and InterventionsKeeshia Mae100% (1)
- Flyer IDDW 2022 Updt 28.07.22Document2 pagesFlyer IDDW 2022 Updt 28.07.22Krisna ChandraNo ratings yet
- Syllabus Foodservice-2Document15 pagesSyllabus Foodservice-2Arienda RKNo ratings yet
- Capaian Mutu Respon Time Igd-2Document1,536 pagesCapaian Mutu Respon Time Igd-2Arsyad AkmatulNo ratings yet
- Zinc Deficiency in ChickensDocument6 pagesZinc Deficiency in ChickensShah NawazNo ratings yet
- OSH With GAD 2Document5 pagesOSH With GAD 2JanrayBernalNo ratings yet
- LASIXDocument2 pagesLASIXMill Jan CruzNo ratings yet
- Sika Monotop®-614 HS: Safety Data SheetDocument10 pagesSika Monotop®-614 HS: Safety Data SheetMuhammad Farhan SetyawanNo ratings yet
- Mukt Shabd JournalDocument9 pagesMukt Shabd JournalJustin SebastianNo ratings yet
- Student Exploration: Disease Spread: Vocabulary: Disease, Epidemic, Infect, Infectious Disease, PathogenDocument5 pagesStudent Exploration: Disease Spread: Vocabulary: Disease, Epidemic, Infect, Infectious Disease, PathogenVijay Shankar PrasadNo ratings yet
- Practice Test: Ielts UsaDocument11 pagesPractice Test: Ielts UsajoseNo ratings yet
- Dializer Hollow FiberDocument6 pagesDializer Hollow FiberdinamariaNo ratings yet
- 1 The Philippines Sam Guidelines 2015 Final Print Ready PDFDocument111 pages1 The Philippines Sam Guidelines 2015 Final Print Ready PDFFar SultanNo ratings yet
- Everyday Health Is ImportantDocument2 pagesEveryday Health Is ImportantEllen WrightNo ratings yet
- Minister of Health V TreatmentDocument82 pagesMinister of Health V TreatmentABDOULIENo ratings yet
- MD Community MedicineDocument14 pagesMD Community MedicineAshwini DongreNo ratings yet
- Hridayrog Sarvangi AbhigamDocument286 pagesHridayrog Sarvangi AbhigamMaheshNo ratings yet
- Public Health Internship: Environmental Health and Safety Intern at Berry Global Summer ScottDocument17 pagesPublic Health Internship: Environmental Health and Safety Intern at Berry Global Summer Scottapi-677941383No ratings yet
- Hope 3 Q1 M6Document12 pagesHope 3 Q1 M6Angelo Jess TorrevillaNo ratings yet