You might also like
- DRRM-H Plan Outline and Guide - July2021 WrefsDocument10 pagesDRRM-H Plan Outline and Guide - July2021 WrefsHerbert Dumaoal100% (3)
- DRRM H For 2020Document187 pagesDRRM H For 2020kristine ezpeleta88% (8)
- DRRM H PLAN Template - v4Document41 pagesDRRM H PLAN Template - v4Patrick Magallano100% (2)
- DOH issues policy on disaster risk reduction and management in healthDocument11 pagesDOH issues policy on disaster risk reduction and management in healthM100% (2)
- Local Investment Plan For HealthDocument23 pagesLocal Investment Plan For HealthAce PortgasNo ratings yet
- CY 2022 2024 DOH Devolution Transition PlanDocument480 pagesCY 2022 2024 DOH Devolution Transition PlanThata Thata100% (2)
- DRRM-H Planning Guide - May 10Document79 pagesDRRM-H Planning Guide - May 10Michael Capuyan Jr100% (2)
- Training Packages For Health Emergencies: Health Emergency Response Operations (HERO)Document57 pagesTraining Packages For Health Emergencies: Health Emergency Response Operations (HERO)Rodney Recto LabisNo ratings yet
- Annex D AOP Forms 2022 LCHODocument170 pagesAnnex D AOP Forms 2022 LCHOdondee100% (3)
- LIPHDocument24 pagesLIPHponceNo ratings yet
- FINAL-Guinayangan AOP 2024Document46 pagesFINAL-Guinayangan AOP 2024Myrna OrnedoNo ratings yet
- DRRM-H Advocacy KitDocument32 pagesDRRM-H Advocacy KitERMED OFC R2TMC100% (1)
- The DRRM-H System: (Achieved/ On-Going/ Not Yet Started)Document3 pagesThe DRRM-H System: (Achieved/ On-Going/ Not Yet Started)maria_abigailNo ratings yet
- Annual Operational Plan 2012 NarrativeDocument11 pagesAnnual Operational Plan 2012 NarrativeArianne A ZamoraNo ratings yet
- School Earthquake DrillDocument22 pagesSchool Earthquake Drilljuncos0729No ratings yet
- National Immunization Program: Manual of Procedures Booklet 11Document42 pagesNational Immunization Program: Manual of Procedures Booklet 11Blue PielagoNo ratings yet
- Report on Seminar Submitted by Akshata on MicrogridsDocument12 pagesReport on Seminar Submitted by Akshata on MicrogridsNitin Kakad73% (11)
- 76 Going To The Hairdresser CanDocument13 pages76 Going To The Hairdresser CanOlga AmyNo ratings yet
- So You Think You Can Think Tools For Having Intelligent Conversations and Getting Along PDFDocument227 pagesSo You Think You Can Think Tools For Having Intelligent Conversations and Getting Along PDFChendikato PinasNo ratings yet
- Misubishi Engine S12R-PTADocument90 pagesMisubishi Engine S12R-PTAAnonymous uEt1sNhU7l100% (15)
- 28NM Beol Cu Gap-Fill Challenges For Metal FilmDocument3 pages28NM Beol Cu Gap-Fill Challenges For Metal FilmKwanghoon Ken Kim100% (1)
- DRRM H 2020 ScribdDocument186 pagesDRRM H 2020 ScribdTagubilin JuliusNo ratings yet
- Baliangao DRRM-H 2023-2025 As of Oct 23, 2023 UpdatedDocument92 pagesBaliangao DRRM-H 2023-2025 As of Oct 23, 2023 UpdatedRoel AbricaNo ratings yet
- V.6 No Red Doc M 2-28-22 Am Manilahealth Department Disaster Risk Reduction and Management Plan For Health Copy Copy Copy 2Document215 pagesV.6 No Red Doc M 2-28-22 Am Manilahealth Department Disaster Risk Reduction and Management Plan For Health Copy Copy Copy 2Tondo Health Center May100% (2)
- Manual On The PEN Protocol On The Integrated Management of Hypertension and DiabetesDocument61 pagesManual On The PEN Protocol On The Integrated Management of Hypertension and DiabetesRanda Noray100% (2)
- Abra DRRMH EoDocument3 pagesAbra DRRMH EoPidigan RHUNo ratings yet
- Panamao Rhu 2024 AopDocument206 pagesPanamao Rhu 2024 AopfatimaraaysaNo ratings yet
- QPMC Liph 2019Document69 pagesQPMC Liph 2019JovelleAnneMondragonNo ratings yet
- Final LGU Scorecard Indicators 2012-2016 As of April 19Document22 pagesFinal LGU Scorecard Indicators 2012-2016 As of April 19Arianne A Zamora100% (19)
- DOH HEMS Guidelines on Hospital Alert SystemsDocument6 pagesDOH HEMS Guidelines on Hospital Alert SystemsIna RamosNo ratings yet
- Now DRRM H Plan 2023 2026 New FOR PRINTDocument52 pagesNow DRRM H Plan 2023 2026 New FOR PRINTLorraine Padlan Baysic100% (1)
- Aop 2022 New Form Blood ProgramDocument21 pagesAop 2022 New Form Blood ProgramCHOLABORATORYNo ratings yet
- HRH Pir Template AdditionalDocument12 pagesHRH Pir Template AdditionalFret Ramirez Coronia RN100% (1)
- MNDRS Manual of OperationsDocument34 pagesMNDRS Manual of OperationsPHO AntNo ratings yet
- DohDocument103 pagesDohRapSamputonNo ratings yet
- Canlamay AopDocument43 pagesCanlamay Aopilog ndpNo ratings yet
- AOP-2024-narrative FINALDocument66 pagesAOP-2024-narrative FINALjasper manuelNo ratings yet
- Form 6 - Rapid Health Assessment (Outbreak)Document1 pageForm 6 - Rapid Health Assessment (Outbreak)DELIVERY ROOMNo ratings yet
- DOH SBIRT ClientflowDocument54 pagesDOH SBIRT ClientflowErin SantosNo ratings yet
- Rhu Citizen CharterDocument18 pagesRhu Citizen CharteradrianNo ratings yet
- eFHSIS MANOPSDocument79 pageseFHSIS MANOPSTracy Thompson100% (3)
- HEARS REPORT FormDocument1 pageHEARS REPORT FormBarangay Guinayang San MateoNo ratings yet
- PDNA Trainees Manual - 2022-03-11-10-21-43-AmDocument74 pagesPDNA Trainees Manual - 2022-03-11-10-21-43-Ambogartjose_ray100% (1)
- 6.1 DRRM-H Step 3 Update - Devt of The Plan - Prevention and Mitigation PlanDocument14 pages6.1 DRRM-H Step 3 Update - Devt of The Plan - Prevention and Mitigation PlanFrab Edar100% (1)
- Doctor To The BarriosDocument1 pageDoctor To The BarriosadjarraNo ratings yet
- DOH AO No 2020 0019 Service Delibvey NetworkDocument15 pagesDOH AO No 2020 0019 Service Delibvey NetworkJose Mari F. EsguerraNo ratings yet
- DM No. 2023 0083 Guidelines For The FHSIS Data Validation and Reconciliation - 22feb2023 2Document11 pagesDM No. 2023 0083 Guidelines For The FHSIS Data Validation and Reconciliation - 22feb2023 2Carlen Mae L. YacapinNo ratings yet
- The Health Promotion HandbookDocument63 pagesThe Health Promotion HandbookOnyd Subingsubing100% (1)
- Universal Health Care Act Provides Comprehensive CoverageDocument17 pagesUniversal Health Care Act Provides Comprehensive CoverageJude Avorque Acidre100% (1)
- EOC Trainees Manual - UpdatedDocument56 pagesEOC Trainees Manual - UpdatedMa. Cristina RanadaNo ratings yet
- AOP OPD Finalsituational and GAP AnalysisDocument2 pagesAOP OPD Finalsituational and GAP AnalysisJennylyn GuadalupeNo ratings yet
- Reporting of Diseases and Health Events OrdinanceDocument10 pagesReporting of Diseases and Health Events OrdinanceRacquel FrondaNo ratings yet
- Doh ProgramsDocument246 pagesDoh ProgramsShengxy FerrerNo ratings yet
- DOH Annual CalendarDocument3 pagesDOH Annual Calendarinvictus0446100% (2)
- dm2022 0394Document21 pagesdm2022 0394Arlo Winston De GuzmanNo ratings yet
- (Uhcis) Mou Template 20191120Document12 pages(Uhcis) Mou Template 20191120Jascha Sabar0% (1)
- dm2020 0439 Omnibus Guidelines PDITR PDFDocument44 pagesdm2020 0439 Omnibus Guidelines PDITR PDFCathryn OrlandaNo ratings yet
- FINAL-Guinayangan AOP 2024Document33 pagesFINAL-Guinayangan AOP 2024Myrna Ornedo100% (2)
- LGU Scorecard DC 2022-0273Document96 pagesLGU Scorecard DC 2022-0273Jomelle WongNo ratings yet
- Measles Campaign For Davao Region: October 26 - November 25, 2020Document44 pagesMeasles Campaign For Davao Region: October 26 - November 25, 2020Brai ƏnNo ratings yet
- Ao2019 0046Document11 pagesAo2019 0046jonathan layaNo ratings yet
- DRRR Week 1415Document7 pagesDRRR Week 1415Yuan Jakob NoverasNo ratings yet
- Agencies. Internal and External Department Need To Have A Clear Understanding of BothDocument2 pagesAgencies. Internal and External Department Need To Have A Clear Understanding of BothEdrea MendezNo ratings yet
- APBHP PlanningDocument6 pagesAPBHP Planningmarcamille100% (1)
- Dokument - Pub DRRM H Planning Guide Module 1 Flipbook PDFDocument16 pagesDokument - Pub DRRM H Planning Guide Module 1 Flipbook PDFMohrein H. Ismael VINo ratings yet
- Threat and Hazard Identification and Risk Assessment (THIRA) and Stakeholder Preparedness Review (SPR) GuideDocument44 pagesThreat and Hazard Identification and Risk Assessment (THIRA) and Stakeholder Preparedness Review (SPR) GuidetmtsukataNo ratings yet
- 7dma R9 Covid Cases 20220110Document1 page7dma R9 Covid Cases 20220110Mohrein H. Ismael VINo ratings yet
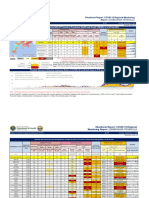
- COVID-19 Regional Report: Zamboanga PeninsulaDocument5 pagesCOVID-19 Regional Report: Zamboanga PeninsulaMohrein H. Ismael VINo ratings yet
- COVID-19 Regional Report: Zamboanga Peninsula Risk LevelsDocument5 pagesCOVID-19 Regional Report: Zamboanga Peninsula Risk LevelsMohrein H. Ismael VINo ratings yet
- 7dma R9 Covid Cases 20210822Document1 page7dma R9 Covid Cases 20210822Mohrein H. Ismael VINo ratings yet
- LDRRMP - Vii AnnexesDocument6 pagesLDRRMP - Vii AnnexesMohrein H. Ismael VINo ratings yet
- LDRRMP - Vi Monitoring and EvaluationDocument19 pagesLDRRMP - Vi Monitoring and EvaluationMohrein H. Ismael VI100% (1)
- Zamboanga Peninsula - Center For Health Development: Annex ADocument1 pageZamboanga Peninsula - Center For Health Development: Annex AMohrein H. Ismael VINo ratings yet
- Dokument - Pub DRRM H Planning Guide Module 1 Flipbook PDFDocument16 pagesDokument - Pub DRRM H Planning Guide Module 1 Flipbook PDFMohrein H. Ismael VINo ratings yet
- LDRRMP - Table of ContentsDocument2 pagesLDRRMP - Table of ContentsMohrein H. Ismael VINo ratings yet
- Certificate Memorandum of Agreement Beyond 22Document1 pageCertificate Memorandum of Agreement Beyond 22Mohrein H. Ismael VINo ratings yet
- Access TB Moa Signing ProgramDocument1 pageAccess TB Moa Signing ProgramMohrein H. Ismael VINo ratings yet
- Access TB Moa Signing ProgramDocument1 pageAccess TB Moa Signing ProgramMohrein H. Ismael VINo ratings yet
- Doh Ao 2020-0022Document17 pagesDoh Ao 2020-0022Mohrein H. Ismael VINo ratings yet
- R55 R-Series 60 HZ FinalDocument2 pagesR55 R-Series 60 HZ FinalCelso Fernandes BentoNo ratings yet
- SQL Plus UsersGuide and Quick ReferenceDocument432 pagesSQL Plus UsersGuide and Quick Referenceapi-25930603No ratings yet
- TITUS Performance Data JET TROWDocument2 pagesTITUS Performance Data JET TROWgeorgeNo ratings yet
- Designing Test Suites: Design A Test Suite For The Following ProblemDocument2 pagesDesigning Test Suites: Design A Test Suite For The Following ProblemAndroid Sourvivors sNo ratings yet
- LogicDocument6 pagesLogicpppppiiiiiNo ratings yet
- Comparison of Rigid Pavement Thickness Design SystemsDocument168 pagesComparison of Rigid Pavement Thickness Design Systemskamalnath100% (1)
- Untitled PresentationDocument14 pagesUntitled PresentationThe BeatableNo ratings yet
- Writing Task 1 - Integrated Question (Test #12) : Your Guide For TOEFL Writing 24+Document3 pagesWriting Task 1 - Integrated Question (Test #12) : Your Guide For TOEFL Writing 24+AstridBarraNo ratings yet
- Everything an Employee Experiences at WorkDocument1 pageEverything an Employee Experiences at WorkAnushka Seth BBA2021MCNo ratings yet
- XX4f ManualDocument480 pagesXX4f ManualEDGAR RICARDONo ratings yet
- Year 4 Geography Field Trip BookletDocument4 pagesYear 4 Geography Field Trip Bookletapi-357287502No ratings yet
- The Validity of Beck Depression Inventory - Short Version in Depressed Patients Diagnosed According To ICD10Document11 pagesThe Validity of Beck Depression Inventory - Short Version in Depressed Patients Diagnosed According To ICD10sarhang talebaniNo ratings yet
- Floriculture Industry in IndiaDocument93 pagesFloriculture Industry in Indiahshah56750% (4)
- Panasonic CX 491 P Datasheet PDFDocument24 pagesPanasonic CX 491 P Datasheet PDFGanesh MandpeNo ratings yet
- Daya Dan Gerakan: Force and MotionDocument21 pagesDaya Dan Gerakan: Force and MotionzinziemeewahNo ratings yet
- 1 SM PDFDocument24 pages1 SM PDFayu sekarNo ratings yet
- Enumerators (x50) - Job Search MalawiDocument4 pagesEnumerators (x50) - Job Search MalawicliftonkacheremNo ratings yet
- Project Time Management and Budget PlanningDocument68 pagesProject Time Management and Budget PlanningLindelani ndalaNo ratings yet
- How To Deal With Multiple SAP Logons - Simple Excel VBADocument14 pagesHow To Deal With Multiple SAP Logons - Simple Excel VBAangel saezNo ratings yet
- Women EmpowermentDocument14 pagesWomen EmpowermentProfessor HappyNo ratings yet
- Hotel Management Ip ProjectDocument36 pagesHotel Management Ip ProjectDivydarshan MishraNo ratings yet
- Surface Safety Products CatalogDocument37 pagesSurface Safety Products CatalogZaid AlahmedNo ratings yet
- Science Flow ChartDocument3 pagesScience Flow ChartEuodia HodeshNo ratings yet
- 8D Report for Broken Snap Ring IssueDocument3 pages8D Report for Broken Snap Ring Issueprabhat sumaNo ratings yet
- Exit StrategyDocument2 pagesExit StrategyMuhammad KashifNo ratings yet