You might also like
- Abnormal PsychologyDocument33 pagesAbnormal PsychologyChristie SabgaNo ratings yet
- CXC Csec English A June 2015 p1Document16 pagesCXC Csec English A June 2015 p1Rihanna Johnson100% (1)
- Vestibular SchwannomasDocument22 pagesVestibular SchwannomasKrisha Anne TaotaoNo ratings yet
- Department of Education: Granja Kalinawan National High SchoolDocument26 pagesDepartment of Education: Granja Kalinawan National High SchoolRoselyn Mae DulaNo ratings yet
- Transdiagnostic TreatmentDocument9 pagesTransdiagnostic Treatmentvalentina chistrugaNo ratings yet
- BD Product ListDocument48 pagesBD Product Listanish_10677953100% (1)
- Complete Holistic Guide To Working Out in The GymDocument218 pagesComplete Holistic Guide To Working Out in The Gympsichi21No ratings yet
- Sarcoidosis DR WinnieDocument33 pagesSarcoidosis DR WinniewinnieNo ratings yet
- Sudden Sensorineural Hearing LossDocument120 pagesSudden Sensorineural Hearing LossprakashoozNo ratings yet
- PMDC Community Medicine Mcqs PDFDocument280 pagesPMDC Community Medicine Mcqs PDFJay KNo ratings yet
- Acoustic Neuroma Acoustic Neuroma & Hearing LossDocument47 pagesAcoustic Neuroma Acoustic Neuroma & Hearing LossArif Nugroho SetiawanNo ratings yet
- Imaging in Brain TumorDocument142 pagesImaging in Brain TumorMagrinov AzaniaNo ratings yet
- Flygt IOM 3152-181Document56 pagesFlygt IOM 3152-181veromesa0% (1)
- Radiology Imaging in Cochlear Implant Preparation PDFDocument50 pagesRadiology Imaging in Cochlear Implant Preparation PDFrizaNo ratings yet
- Acoustic Neuroma Acoustic Neuroma & Hearing LossDocument48 pagesAcoustic Neuroma Acoustic Neuroma & Hearing LosstaqadasabbasNo ratings yet
- Thyroid Ultrasound Basic: ATA Fellow Track 2013Document26 pagesThyroid Ultrasound Basic: ATA Fellow Track 2013Yav KNo ratings yet
- Otosclerosis: Pathogenesis & ManagementDocument112 pagesOtosclerosis: Pathogenesis & Managementanon_205487480No ratings yet
- Acoustic NeuromaDocument33 pagesAcoustic NeuromahafizNo ratings yet
- Otosclerosis Presentation MBBSDocument119 pagesOtosclerosis Presentation MBBSFaltuNo ratings yet
- The Diagnostic and Etiological Contribution of Sectional Imaging in Deafness (About 80 Cases)Document7 pagesThe Diagnostic and Etiological Contribution of Sectional Imaging in Deafness (About 80 Cases)IJAR JOURNALNo ratings yet
- Incidence of Recurrent Laryngeal Nerve Palsy Following Thyroid SurgeryDocument25 pagesIncidence of Recurrent Laryngeal Nerve Palsy Following Thyroid SurgeryAshokNo ratings yet
- Barrs 2001Document22 pagesBarrs 2001AshokNo ratings yet
- Otosclerosis Slides 061018Document96 pagesOtosclerosis Slides 061018Paraguay De La Cruz JoelNo ratings yet
- Vestibular Schwannoma (Acoustic Neuroma) - UpToDateDocument26 pagesVestibular Schwannoma (Acoustic Neuroma) - UpToDateanton MDNo ratings yet
- A Normative Study of Tympanic Membrane Motion in Humans Using A Laser Doppler Vibrometer (LDV)Document20 pagesA Normative Study of Tympanic Membrane Motion in Humans Using A Laser Doppler Vibrometer (LDV)g mailNo ratings yet
- Incidence of RLN Palsy Thyroid Surgery at BSMMUDocument25 pagesIncidence of RLN Palsy Thyroid Surgery at BSMMUAshokNo ratings yet
- Nutrimentum Vascularum As Pulsatile TinnitusDocument6 pagesNutrimentum Vascularum As Pulsatile TinnitusJuthika Rai ShettyNo ratings yet
- Incidence of Recurrent Laryngeal Nerve Palsy Following Thyroid SurgeryDocument21 pagesIncidence of Recurrent Laryngeal Nerve Palsy Following Thyroid SurgeryAshokNo ratings yet
- A Clinical Study of Sudden DeafnessDocument7 pagesA Clinical Study of Sudden Deafnesswildan yogaNo ratings yet
- "Pediatric Radiation Oncology": R. Miralbell Hôpitaux Universitaires, GenèveDocument118 pages"Pediatric Radiation Oncology": R. Miralbell Hôpitaux Universitaires, GenèveRus Paul OvidiuNo ratings yet
- Head & Neck Case Study: Parotid Gland: Alyssa MellottDocument28 pagesHead & Neck Case Study: Parotid Gland: Alyssa Mellottapi-281921437No ratings yet
- Cervical DystoniaDocument5 pagesCervical DystoniaOmar ElsahartyNo ratings yet
- The Sensitivity of Auditory Brainstem Response Testing For The Diagnosis of Acoustic NeuromasDocument4 pagesThe Sensitivity of Auditory Brainstem Response Testing For The Diagnosis of Acoustic NeuromasSekti JsiNo ratings yet
- Neck Pain 3Document8 pagesNeck Pain 3natasyaNo ratings yet
- Neuro4Nurses Acustic NeuromaDocument2 pagesNeuro4Nurses Acustic Neuromaputri auliyahNo ratings yet
- 03 - A Study On Peripheral Vertigo in A Kolkata Based Hospital PDFDocument4 pages03 - A Study On Peripheral Vertigo in A Kolkata Based Hospital PDFShivaam KesarwaaniNo ratings yet
- Inter of CXR & Rad ProtectionDocument91 pagesInter of CXR & Rad ProtectionS B SayedNo ratings yet
- Radiosurgery in Brain Tumours: DR Debnarayan Dutta, MDDocument52 pagesRadiosurgery in Brain Tumours: DR Debnarayan Dutta, MDs024No ratings yet
- Nasopharyngeal Carcinoma: M. Ivan DjajalagaDocument83 pagesNasopharyngeal Carcinoma: M. Ivan DjajalagaRytma RiyanthiNo ratings yet
- 12 Bone and Soft Tissue Sarcomas 200609 v2Document58 pages12 Bone and Soft Tissue Sarcomas 200609 v2dr. Ahmad MuhsininNo ratings yet
- Pediatric - Hearing - Loss Lau 3-17-10Document45 pagesPediatric - Hearing - Loss Lau 3-17-10Arief FakhrizalNo ratings yet
- B1 PDFDocument6 pagesB1 PDFDr. Arvind YadavNo ratings yet
- Hearing Loss - Could It Be Usher Syndrome - PPTX 1.14.13for Posting To WebDocument41 pagesHearing Loss - Could It Be Usher Syndrome - PPTX 1.14.13for Posting To WebrajaalfatihNo ratings yet
- Berg RRP TalkDocument39 pagesBerg RRP TalkΕμμανουήλ ΚακαβελάκηςNo ratings yet
- NCRP 160 PDFDocument81 pagesNCRP 160 PDFmarkNo ratings yet
- Cochlear Implantation in Postlingually Deaf Adults Is Time-Sensitive Towards Positive Outcome: Prediction Using Advanced Machine Learning TechniquesDocument9 pagesCochlear Implantation in Postlingually Deaf Adults Is Time-Sensitive Towards Positive Outcome: Prediction Using Advanced Machine Learning TechniquesXilena HerreraNo ratings yet
- Schwannoma Vestibular TinnitusDocument6 pagesSchwannoma Vestibular TinnitusThomasMáximoMancinelliRinaldoNo ratings yet
- Caeliac Hearing LossDocument6 pagesCaeliac Hearing LossgyaiffNo ratings yet
- Raynaud's Phenomenon, Vibration Induced White Finger, and Difficulties in HearingDocument3 pagesRaynaud's Phenomenon, Vibration Induced White Finger, and Difficulties in HearingDhakves JustikaNo ratings yet
- Utility of Mri in The Early and Accurate Diagnosis of Avascular Necrosis of Hip JointDocument9 pagesUtility of Mri in The Early and Accurate Diagnosis of Avascular Necrosis of Hip JointDenis AlexandruNo ratings yet
- Diagnosis and Classification in MRI of Brucellar SpondylitisDocument6 pagesDiagnosis and Classification in MRI of Brucellar SpondylitisMANGNo ratings yet
- The Role of Post-RT FDG PET in Neck Dissection For Regionally Advanced Head and Neck Cancer (PDFDrive)Document165 pagesThe Role of Post-RT FDG PET in Neck Dissection For Regionally Advanced Head and Neck Cancer (PDFDrive)Bianca DanielaNo ratings yet
- Unilateral Vocal Cord ParalysisDocument41 pagesUnilateral Vocal Cord ParalysisDrravikumar BhandariNo ratings yet
- Journal 1Document6 pagesJournal 1Widyasari WuwunganNo ratings yet
- Radio Logical Diagnosis of Horn CancerDocument2 pagesRadio Logical Diagnosis of Horn CancereditorveterinaryworldNo ratings yet
- Lupus Case Study Part 3Document20 pagesLupus Case Study Part 3Mykee SuizoNo ratings yet
- Metastaticeurospine2015 151207184233 Lva1 App6891Document122 pagesMetastaticeurospine2015 151207184233 Lva1 App6891niluhputu asrinidewiNo ratings yet
- Referensi Tesis Spesialis DrumondDocument8 pagesReferensi Tesis Spesialis DrumondflorensiaNo ratings yet
- Hearing Disorders in StrokeDocument15 pagesHearing Disorders in Strokeveerraju tvNo ratings yet
- 17 Neoplasms of The EarDocument49 pages17 Neoplasms of The Earsunil paiNo ratings yet
- Scrotal PainDocument7 pagesScrotal PainPipitNo ratings yet
- Meniers DsDocument59 pagesMeniers DsAnurag SrivastavaNo ratings yet
- Cerebellopontine Angle TumoursDocument11 pagesCerebellopontine Angle TumoursIsmail Sholeh Bahrun MakkaratteNo ratings yet
- Diffuse Astrocytomas: Dr. Samuel OlukaDocument29 pagesDiffuse Astrocytomas: Dr. Samuel OlukaSam OlukaNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFLopez C PaulNo ratings yet
- Extensive Intratemporal Cholesteatoma: Surgical StrategyDocument8 pagesExtensive Intratemporal Cholesteatoma: Surgical Strategydisk_la_poduNo ratings yet
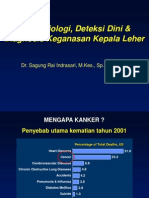
- Epidemiologi, Deteksi Dini & Diagnosis Keganasan Kepala LeherDocument37 pagesEpidemiologi, Deteksi Dini & Diagnosis Keganasan Kepala LeherRuki HartawanNo ratings yet
- Temporal Bone CancerFrom EverandTemporal Bone CancerPaul W. GidleyNo ratings yet
- Wipe Sampling Materials For Lead in Surface DustDocument3 pagesWipe Sampling Materials For Lead in Surface DustAhmad Zubair RasulyNo ratings yet
- HSC 430 - Lesson Plan Underage DrinkingDocument11 pagesHSC 430 - Lesson Plan Underage Drinkingapi-487139726No ratings yet
- Neurobic Excersise Impact On Cognative FunctionDocument8 pagesNeurobic Excersise Impact On Cognative FunctionZalinah Mohd YusofNo ratings yet
- Test Bank For Mosbys Essentials For Nursing Assistants 4th Edition SorrentinoDocument24 pagesTest Bank For Mosbys Essentials For Nursing Assistants 4th Edition Sorrentinozacharymcleanpdqogjyfeb100% (47)
- Persona Partial Knee Brochure PDFDocument12 pagesPersona Partial Knee Brochure PDF洪侊增No ratings yet
- Microbial Limits Tests: The Difference Between "Absence of Objectionable Microorganisms" and "Absence of Specified Microorganisms"Document7 pagesMicrobial Limits Tests: The Difference Between "Absence of Objectionable Microorganisms" and "Absence of Specified Microorganisms"Jai MurugeshNo ratings yet
- A Chance To Save Millions of Lives by Freeing Up Drug Patents - Advanced PDFDocument5 pagesA Chance To Save Millions of Lives by Freeing Up Drug Patents - Advanced PDFhahahapsuNo ratings yet
- Liver Vascular Anatomy - A RefresherDocument10 pagesLiver Vascular Anatomy - A Refresherilham nugrohoNo ratings yet
- Policy That Implemented in Kota SamarahanDocument9 pagesPolicy That Implemented in Kota SamarahanIskandar IskandarNo ratings yet
- Common Causes of Calf Pain in Endurance Athletes: by Brad J. Bernardini, MD, FAAOS, Reconstructive OrthopedicsDocument2 pagesCommon Causes of Calf Pain in Endurance Athletes: by Brad J. Bernardini, MD, FAAOS, Reconstructive Orthopedicsbila inunNo ratings yet
- Assignment: Name: Qolbu Adi Wicaksono NIM: 19109011014Document3 pagesAssignment: Name: Qolbu Adi Wicaksono NIM: 19109011014Hafshah AgustinaNo ratings yet
- KSCST PresentationDocument44 pagesKSCST PresentationAkshay SavvasheriNo ratings yet
- House Bill 15-1043Document19 pagesHouse Bill 15-1043Michael_Lee_RobertsNo ratings yet
- Iap Guidelines On Rickettsial Diseases in ChildrenDocument7 pagesIap Guidelines On Rickettsial Diseases in Childrenitaa19No ratings yet
- Uu No. 16 Tahun 1992Document120 pagesUu No. 16 Tahun 1992Nanda Yusuf Dwi PNo ratings yet
- Respaper 1Document48 pagesRespaper 1Xayezi AblenNo ratings yet
- Ion Breeding Policy - 2006 & 2010Document42 pagesIon Breeding Policy - 2006 & 2010Ulhas GaikwadNo ratings yet
- ARC 360 NGP InstructionManualDocument24 pagesARC 360 NGP InstructionManualLMTNo ratings yet
- Rajasthan Hospitals LISTDocument19 pagesRajasthan Hospitals LISTOrigin Over100% (1)
- Art Comparison Essay ExampleDocument5 pagesArt Comparison Essay Exampleflrzcpaeg100% (2)
- Assessment of PersonalityDocument3 pagesAssessment of PersonalityRahman ButtNo ratings yet