You might also like
- Dr. Najeeb NephrologyDocument53 pagesDr. Najeeb NephrologyTrajce100% (3)
- Science 8 PDFDocument172 pagesScience 8 PDFaftab khanNo ratings yet
- Urinary SystemDocument9 pagesUrinary SystemCailah Sofia SelausoNo ratings yet
- Assessment or Acute Renal Failure SymptomsDocument6 pagesAssessment or Acute Renal Failure SymptomsRifa Aprillia CahyaniNo ratings yet
- Diabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Chronic Kidney DiseaseDocument6 pagesChronic Kidney Diseaseashi leginNo ratings yet
- Feline Urologic Syndrome enDocument2 pagesFeline Urologic Syndrome enSitiNurjannahNo ratings yet
- Renal Function TestDocument27 pagesRenal Function TestKuzhandai Velu50% (2)
- Renal PhysiologyDocument124 pagesRenal Physiologynirilib100% (2)
- Health TeachingsDocument7 pagesHealth Teachingstheamacias100% (2)
- Renal Function TestsDocument28 pagesRenal Function TestsAbeer Ahmed100% (1)
- Clinical Science Session on Acute Kidney InjuryDocument16 pagesClinical Science Session on Acute Kidney Injuryirwan50% (2)
- Acute Kidney Injury - Chronic Kidney DeseaseDocument71 pagesAcute Kidney Injury - Chronic Kidney DeseaseFina Ahmad Fitriana100% (1)
- Lab (5) Creatinine Clearance&GFRDocument16 pagesLab (5) Creatinine Clearance&GFRAkshay Chandra Vemulapalli100% (1)
- Chronic Kidney DiseaseDocument8 pagesChronic Kidney DiseaseIndhumathiNo ratings yet
- Renal FunctionsDocument30 pagesRenal FunctionsJay Andrea Vea Israel100% (1)
- Renal Function TestsDocument23 pagesRenal Function TestsKer YehunNo ratings yet
- Acute Renal FailureDocument4 pagesAcute Renal FailurePerrilyn PereyNo ratings yet
- Renal Function TestsDocument36 pagesRenal Function TestsLawal Bello DanchadiNo ratings yet
- Kidney Function TestsDocument15 pagesKidney Function Testspntmai.y2020No ratings yet
- Veterinary medicine faculty renal function testsDocument7 pagesVeterinary medicine faculty renal function testsMustafa El-saeedNo ratings yet
- Ren Function TestDocument10 pagesRen Function TestSankha DasNo ratings yet
- Acute Renal Failure Nursing CareDocument85 pagesAcute Renal Failure Nursing Careellise abundoNo ratings yet
- 4 BodyDocument35 pages4 Bodysinte beyuNo ratings yet
- Clinical Chemistry Lec 5Document70 pagesClinical Chemistry Lec 5salamshakir56No ratings yet
- L2 - Disorders of The Kidney and Urinary TractDocument35 pagesL2 - Disorders of The Kidney and Urinary TractAhmad SobihNo ratings yet
- Lab 4 5 Renal Functions TestDocument6 pagesLab 4 5 Renal Functions TestMustafa MahdiNo ratings yet
- Abeer Renal Function Testsamr Renal Function Tests Renal BlockDocument22 pagesAbeer Renal Function Testsamr Renal Function Tests Renal BlockAbeer AhmedNo ratings yet
- المحاطرة الاولة كيمياء سريريةDocument35 pagesالمحاطرة الاولة كيمياء سريريةMohamedErrmaliNo ratings yet
- Kidney Function TestsDocument36 pagesKidney Function TestsAmbreen MurtazaNo ratings yet
- Kidney DisorderDocument94 pagesKidney DisorderBok MatthewNo ratings yet
- Acute Kidney Injury and Chronic Kidney DiseaseDocument44 pagesAcute Kidney Injury and Chronic Kidney DiseaseIda Bagus Putu Swabawa100% (1)
- Screenshot 2023-10-17 at 11.20.08 AMDocument3 pagesScreenshot 2023-10-17 at 11.20.08 AMs8903082No ratings yet
- Renal Function Test Amcj 8Document42 pagesRenal Function Test Amcj 8Md. Saifur Rahman SunnyNo ratings yet
- Renal Function TestDocument36 pagesRenal Function TestPoomuhi sathasivamNo ratings yet
- Drugs Therapy For Kidney: Budi RaharjoDocument33 pagesDrugs Therapy For Kidney: Budi RaharjoNurul MasyithahNo ratings yet
- Acute Kidney FailureDocument2 pagesAcute Kidney FailureKunjan ShahNo ratings yet
- Renal Function TestDocument5 pagesRenal Function Testmitchelleizzy100% (1)
- L2 InvestigationDocument14 pagesL2 InvestigationMohammed A. JameelNo ratings yet
- Azotemia: Understanding Causes and Pathophysiology of Elevated BUN and CreatinineDocument25 pagesAzotemia: Understanding Causes and Pathophysiology of Elevated BUN and CreatininePrajna PNo ratings yet
- Integral University, Lucknow: Session:2019-2020Document6 pagesIntegral University, Lucknow: Session:2019-2020Kausal VermaNo ratings yet
- FrancesFranciscoCC2 1Document6 pagesFrancesFranciscoCC2 1Frances FranciscoNo ratings yet
- 2D2016 3.4-2 Azotemia and Urinary Abnormalities (Harrison's)Document7 pages2D2016 3.4-2 Azotemia and Urinary Abnormalities (Harrison's)elleinas100% (1)
- Akd & CKDDocument44 pagesAkd & CKDﻣﻠﻚ عيسىNo ratings yet
- Non-Protein Nitrogen CompoundsDocument6 pagesNon-Protein Nitrogen CompoundspixiedustNo ratings yet
- Reagent StripDocument7 pagesReagent Stripromerodion71No ratings yet
- Lecture (5) Kidney Function Tests Part IDocument33 pagesLecture (5) Kidney Function Tests Part IAmine GobranNo ratings yet
- Renal failure diet guidelines for nephrotic syndromeDocument73 pagesRenal failure diet guidelines for nephrotic syndromeNurul AlfatarisyaNo ratings yet
- Uremic Syndrome - Acut Kidney Injury - Chronic Kidney DiseaseDocument28 pagesUremic Syndrome - Acut Kidney Injury - Chronic Kidney DiseaseZikri Putra Lan LubisNo ratings yet
- Kidney Function Tests 2Document30 pagesKidney Function Tests 2kamalNo ratings yet
- Gagal Ginjal Akut & Gagal Ginjal KronikDocument63 pagesGagal Ginjal Akut & Gagal Ginjal KronikSuf YusufNo ratings yet
- Evaluation of Kidney FunctionDocument29 pagesEvaluation of Kidney FunctionAoiNo ratings yet
- REVIEW 2023 AUBF Basics On Chemical Tests For UrineDocument84 pagesREVIEW 2023 AUBF Basics On Chemical Tests For UrineJheshari VinaNo ratings yet
- Fluid and Electrolytes Assignment 1. What Are The Different Processes of Body Fluid and Solutes Movement? and Give at Least 2 Examples EachDocument8 pagesFluid and Electrolytes Assignment 1. What Are The Different Processes of Body Fluid and Solutes Movement? and Give at Least 2 Examples EachAngelicaNo ratings yet
- Fluid and Electrolytes Assignment 1. What Are The Different Processes of Body Fluid and Solutes Movement? and Give at Least 2 Examples EachDocument8 pagesFluid and Electrolytes Assignment 1. What Are The Different Processes of Body Fluid and Solutes Movement? and Give at Least 2 Examples EachAngelicaNo ratings yet
- Renal Function Tests: Understanding BUN, Creatinine, and ClearanceDocument26 pagesRenal Function Tests: Understanding BUN, Creatinine, and ClearanceHarshini MakkenaNo ratings yet
- Antibiotics Hemoglobin: SodiumDocument5 pagesAntibiotics Hemoglobin: Sodiumlouie roderosNo ratings yet
- Renal Function Test (RFT) : Muhammad Asif Shaheen Lecturer Pathology Kemu, LahoreDocument14 pagesRenal Function Test (RFT) : Muhammad Asif Shaheen Lecturer Pathology Kemu, LahoreRimsha MustafaNo ratings yet
- HTTPDocument10 pagesHTTPkasmiatiNo ratings yet
- Renal ClearanceDocument35 pagesRenal ClearanceSamudrala VijaykumarNo ratings yet
- Renal Fuction TestsDocument57 pagesRenal Fuction Testsmirabel IvanaliNo ratings yet
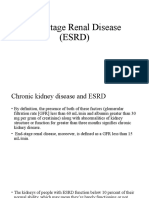
- End Stage Renal Disease (ESRD)Document21 pagesEnd Stage Renal Disease (ESRD)Dani DanyNo ratings yet
- Renal Function Tests: BUN, Creatinine & ClearanceDocument29 pagesRenal Function Tests: BUN, Creatinine & ClearanceRoshan KumarNo ratings yet
- NPNDocument42 pagesNPNreynanrolleNo ratings yet
- L4 KFTsDocument4 pagesL4 KFTsRobin TikhatriNo ratings yet
- Kidney Function TestDocument30 pagesKidney Function TestSrikrishnaNo ratings yet
- 7-Blood GroupDocument22 pages7-Blood GroupCabdalle KurbeNo ratings yet
- Basic measurements in epidemiologyDocument58 pagesBasic measurements in epidemiologyCabdalle KurbeNo ratings yet
- (Handout) Introduction To Research MethodologyDocument6 pages(Handout) Introduction To Research MethodologyCabdalle KurbeNo ratings yet
- Introduction To EpidemiologyDocument44 pagesIntroduction To EpidemiologyCabdalle KurbeNo ratings yet
- Blood Culture CollectionDocument18 pagesBlood Culture CollectionLiz Escueta100% (1)
- 2 - Serological TechniquesDocument10 pages2 - Serological TechniquesCabdalle KurbeNo ratings yet
- Blood Grouping: E Mtenan H As SanDocument22 pagesBlood Grouping: E Mtenan H As SanCabdalle KurbeNo ratings yet
- ABO Blood Group System: Alaa Ibrahim Mohammed Hassan Lecturer of Haematology & Immunohaematology FMLS, U of KDocument50 pagesABO Blood Group System: Alaa Ibrahim Mohammed Hassan Lecturer of Haematology & Immunohaematology FMLS, U of KCabdalle KurbeNo ratings yet
- Detect Sensitized RBCs & Antibodies with DAT, IAT & Du TestsDocument4 pagesDetect Sensitized RBCs & Antibodies with DAT, IAT & Du TestsCabdalle KurbeNo ratings yet
- Blood Grouping: E Mtenan H As SanDocument22 pagesBlood Grouping: E Mtenan H As SanCabdalle KurbeNo ratings yet
- Measure bleeding and clotting timesDocument3 pagesMeasure bleeding and clotting timesCabdalle KurbeNo ratings yet
- Measure bleeding and clotting timesDocument3 pagesMeasure bleeding and clotting timesCabdalle KurbeNo ratings yet
- 2 - Serological TechniquesDocument10 pages2 - Serological TechniquesCabdalle KurbeNo ratings yet
- ABO Blood Group System: Alaa Ibrahim Mohammed Hassan Lecturer of Haematology & Immunohaematology FMLS, U of KDocument50 pagesABO Blood Group System: Alaa Ibrahim Mohammed Hassan Lecturer of Haematology & Immunohaematology FMLS, U of KCabdalle KurbeNo ratings yet
- 4-DAT, IDAT and Du MethodDocument4 pages4-DAT, IDAT and Du MethodCabdalle KurbeNo ratings yet
- Renal System Components FunctionsDocument3 pagesRenal System Components FunctionsJohn Juan TwanNo ratings yet
- Analysis of Abnormal Constituents of UrineDocument20 pagesAnalysis of Abnormal Constituents of UrineDhanalakshmiNo ratings yet
- RUMUSDocument1 pageRUMUSdevinaNo ratings yet
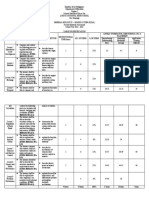
- Table of Specification (REVISED)Document2 pagesTable of Specification (REVISED)Rodel Somera TabanNo ratings yet
- Urinary System Review QuestionsDocument3 pagesUrinary System Review QuestionsSaajid AmraNo ratings yet
- Renal Dysplasia in DogsDocument6 pagesRenal Dysplasia in DogsThalita EmilyNo ratings yet
- Advances in Understanding The Urine-Concentrating MechanismDocument26 pagesAdvances in Understanding The Urine-Concentrating MechanismKiara Lopez RelaizaNo ratings yet
- Group Health Insurance Proposal Form for Bajaj Allianz General InsuranceDocument3 pagesGroup Health Insurance Proposal Form for Bajaj Allianz General InsuranceDenver SaldanhaNo ratings yet
- Kidney Failure (Reference Summary) : AnatomyDocument3 pagesKidney Failure (Reference Summary) : AnatomyUSMP FN ARCHIVOSNo ratings yet
- Excrection 1Document18 pagesExcrection 1Liyana AziziNo ratings yet
- X Life-Processes Excretion Module 1 of 3Document7 pagesX Life-Processes Excretion Module 1 of 3Tharika MahendranNo ratings yet
- Long-Term Safety and Efficacy of Psoas Bladder Hitch in Infants Aged Menor 12 Months With Unilateral Obstructive Megaureter. 2020. ENSAYO CLINICODocument8 pagesLong-Term Safety and Efficacy of Psoas Bladder Hitch in Infants Aged Menor 12 Months With Unilateral Obstructive Megaureter. 2020. ENSAYO CLINICOJulio GomezNo ratings yet
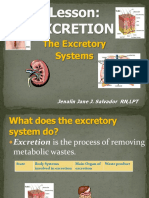
- ExcretionDocument39 pagesExcretionJennifer J. Pascua100% (1)
- Chapter 15 JK PDFDocument47 pagesChapter 15 JK PDFCitra Aulia BachtiarNo ratings yet
- Urine Analysis: Review of Literature Chapter 2Document11 pagesUrine Analysis: Review of Literature Chapter 2Ahmed Naguib MohamedNo ratings yet
- Detecting urine components with reagent stripsDocument24 pagesDetecting urine components with reagent stripspat bNo ratings yet
- AUBF Reinforcement ExamDocument67 pagesAUBF Reinforcement ExamVanessa May BlancioNo ratings yet
- MCH Urology Dissertation TopicsDocument7 pagesMCH Urology Dissertation TopicsBuyAPaperOnlineBaltimore100% (1)
- Kidney Anatomy and Function OverviewDocument13 pagesKidney Anatomy and Function OverviewHannah Grace GalinatoNo ratings yet
- Renal Ultrasound ProtocolDocument4 pagesRenal Ultrasound Protocolfouad tabetNo ratings yet
- The circulatory and excretory systems in humansDocument12 pagesThe circulatory and excretory systems in humanssuvashreeNo ratings yet
- Mcu Test Micturating CystourethrogramDocument1 pageMcu Test Micturating CystourethrogramSudharsanNo ratings yet
- Cardinal Manifestetions of Renal DiseaseDocument61 pagesCardinal Manifestetions of Renal Diseasekirubel deribNo ratings yet