You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Prosecutor's HandbookDocument162 pagesThe Prosecutor's HandbooksamuelNo ratings yet
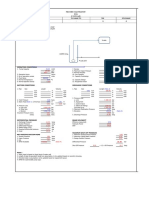
- Pump Sizing SpreadsheetDocument2 pagesPump Sizing Spreadsheetandrew rachmanNo ratings yet
- Spirax-Sarco - Boiler Controls and SystemsDocument8 pagesSpirax-Sarco - Boiler Controls and SystemstpqnhatNo ratings yet
- Aclu List Research Export 20160810050210Document2 pagesAclu List Research Export 20160810050210api-285701682100% (1)
- Bulk Solids HandlingDocument303 pagesBulk Solids HandlingDr_M_Soliman100% (12)
- Battery Calculations For Fire Alarm and Signaling SystemsDocument7 pagesBattery Calculations For Fire Alarm and Signaling Systemsleland macasinag100% (1)
- Percutaneous Coronary Intervention 10 05Document8 pagesPercutaneous Coronary Intervention 10 05benypermadiNo ratings yet
- Acute Limb Ischemia SiteDocument23 pagesAcute Limb Ischemia Sitebenypermadi100% (1)
- Acute Limb Ischemia SiteDocument23 pagesAcute Limb Ischemia Sitebenypermadi100% (1)
- ACFCS Certification BrochureDocument7 pagesACFCS Certification Brochurebeena pandeyNo ratings yet
- How Nokia Failed to Adapt to Market ChangesDocument5 pagesHow Nokia Failed to Adapt to Market ChangesRiangelli ExcondeNo ratings yet
- Pci Stent CaringDocument5 pagesPci Stent CaringbenypermadiNo ratings yet
- Nursing Care for Coronary Intervention: Primary PCIDocument10 pagesNursing Care for Coronary Intervention: Primary PCIbenypermadiNo ratings yet
- Care of The Post PICA (Stent)Document75 pagesCare of The Post PICA (Stent)benypermadiNo ratings yet
- CT Coronary AnatomyDocument68 pagesCT Coronary AnatomybenypermadiNo ratings yet
- Openhrt 2021 001732Document9 pagesOpenhrt 2021 001732benypermadiNo ratings yet
- CT Coronary AnatomyDocument68 pagesCT Coronary AnatomybenypermadiNo ratings yet
- Sat 1315-1415 Cardiac AngiogDocument47 pagesSat 1315-1415 Cardiac AngiogbenypermadiNo ratings yet
- Openhrt 2021 001732Document9 pagesOpenhrt 2021 001732benypermadiNo ratings yet
- Coronary Circulation: - Dr. ChintanDocument42 pagesCoronary Circulation: - Dr. ChintanbenypermadiNo ratings yet
- M6. L2 Optimal Care Post InterventionDocument25 pagesM6. L2 Optimal Care Post InterventionbenypermadiNo ratings yet
- Setting The Pace: Pacemaker Principles: AcknowledgementsDocument40 pagesSetting The Pace: Pacemaker Principles: AcknowledgementsbenypermadiNo ratings yet
- Cardiovascular ImagingDocument32 pagesCardiovascular ImagingSunn Ren TeeNo ratings yet
- Toaz - Info Module in Ergonomics and Planning Facilities For The Hospitality Industry PRDocument33 pagesToaz - Info Module in Ergonomics and Planning Facilities For The Hospitality Industry PRma celine villoNo ratings yet
- 1.3 Swot and PDP AnalysisDocument4 pages1.3 Swot and PDP AnalysismiroyNo ratings yet
- To Register Your IGP Please Visit or Scan The QR Code Below To Register Your IGP Please Visit or Scan The QR Code BelowDocument1 pageTo Register Your IGP Please Visit or Scan The QR Code Below To Register Your IGP Please Visit or Scan The QR Code BelowLester Jao SegubanNo ratings yet
- Elite Physics G10 T2 SLA1Document7 pagesElite Physics G10 T2 SLA1thecubeg0No ratings yet
- HistoryDocument13 pagesHistoryMuhamed Zimić ZimaNo ratings yet
- 20 5880100Document2 pages20 5880100'Theodora GeorgianaNo ratings yet
- College of Industrial Technology Bachelor of Technology and Livelihood Education (TLE) CMO. No. 78, S. 2017Document5 pagesCollege of Industrial Technology Bachelor of Technology and Livelihood Education (TLE) CMO. No. 78, S. 2017Industrial TechnologyNo ratings yet
- Excel - Bachelorprojekt - Bertil Theis JørgensenDocument944 pagesExcel - Bachelorprojekt - Bertil Theis JørgensenBertil JørgensenNo ratings yet
- Datasheet of DS 7608NI Q1 - 8P NVRD - V4.71.200 - 20220705Document5 pagesDatasheet of DS 7608NI Q1 - 8P NVRD - V4.71.200 - 20220705Gherel TocasNo ratings yet
- Ultra Life ER14250 DatasheetDocument2 pagesUltra Life ER14250 DatasheetArslan AwanNo ratings yet
- Sap AbapDocument7 pagesSap Abapidrees aliNo ratings yet
- Function-Answer (2016-2018)Document9 pagesFunction-Answer (2016-2018)朱瑞霖No ratings yet
- Nurses' Documentation of Falls Prevention in A Patient Centred Care Plan in A Medical WardDocument6 pagesNurses' Documentation of Falls Prevention in A Patient Centred Care Plan in A Medical WardJAY LORRAINE PALACATNo ratings yet
- Electrical Machine 7-26-2016Document94 pagesElectrical Machine 7-26-2016Engr. Raheel khanNo ratings yet
- What Is A Human Resources Strategy?Document8 pagesWhat Is A Human Resources Strategy?abdallah abdNo ratings yet
- Certificate of Analysis - Certified Reference Material: Cetyl PalmitateDocument6 pagesCertificate of Analysis - Certified Reference Material: Cetyl PalmitateRachel McArdleNo ratings yet
- National Electrification Administration Vs GonzagaDocument1 pageNational Electrification Administration Vs GonzagaDonna Amethyst BernardoNo ratings yet
- Case Study - NISSANDocument5 pagesCase Study - NISSANChristy BuiNo ratings yet
- Corbin Technical Bulletin Volume 4Document149 pagesCorbin Technical Bulletin Volume 4aikidomoysesNo ratings yet
- SDA HLD Template v1.3Document49 pagesSDA HLD Template v1.3Samuel TesfayeNo ratings yet
- Assignment 2Document21 pagesAssignment 2api-445531772No ratings yet
- REMMLOTDocument53 pagesREMMLOTarpit saraswat100% (1)