You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Precision, Recall, F1-ScoreDocument6 pagesPrecision, Recall, F1-ScoreKesehoNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- ABB Surge Arresters 2019-10-17Document132 pagesABB Surge Arresters 2019-10-17sanjeev banerjeeNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Teacher Standard 4 - BrandedDocument2 pagesTeacher Standard 4 - BrandedPaul DuiunovNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- OscillatorsDocument3 pagesOscillatorsDanley Rodrigues DantasNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 10 DOH Approved Herbal MDocument4 pages10 DOH Approved Herbal MKarl Kiw-isNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- EVS Assignment Question by Vedant Nagpal Answer 03Document1 pageEVS Assignment Question by Vedant Nagpal Answer 03Vedant NagpalNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Engineering Assistant in Prasar Bharti 2013 Final Result PDFDocument27 pagesEngineering Assistant in Prasar Bharti 2013 Final Result PDFKiran Jot SinghNo ratings yet
- Evolution of Music Players - Group 2 MusicDocument17 pagesEvolution of Music Players - Group 2 MusicLinda AgmataNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Government Game Student WorksheetDocument3 pagesThe Government Game Student WorksheetAnuj Singh BhadoriyaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- ReportDocument33 pagesReportBhavesh JoliyaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Blueprint Reading SyllabusDocument5 pagesBlueprint Reading SyllabusceskeenNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- PRE4Document105 pagesPRE4J. BautistaNo ratings yet
- Main Duties and ResponsibilitiesDocument3 pagesMain Duties and ResponsibilitiessafiullahNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- ChemistryDocument16 pagesChemistryShashank Dubey0% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- PHP Cheat SheetDocument2 pagesPHP Cheat SheetEsha ShahNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Chrystal Chao Ci Xin'赵: Achievements Software SkillsDocument4 pagesChrystal Chao Ci Xin'赵: Achievements Software SkillsCHAO CI XINNo ratings yet
- IOQ of MetrixDocument36 pagesIOQ of Metrixmkm969No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Research Journal of Internatıonal StudıesDocument16 pagesResearch Journal of Internatıonal StudıesShamsher ShirazNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- English Malay DictionaryDocument614 pagesEnglish Malay DictionaryGanesh Balaji100% (1)
- DLP VIII How Land Masses and Bodies of Water Affects The TyphoonDocument5 pagesDLP VIII How Land Masses and Bodies of Water Affects The TyphoonNellen Bastismo100% (1)
- Prosper - Tutorial - 00 by CIMA-TQDocument87 pagesProsper - Tutorial - 00 by CIMA-TQPedro MarquezNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Language Applied To Volcanic ParticlesDocument3 pagesLanguage Applied To Volcanic Particlesjunior.geologiaNo ratings yet
- HAREDA PAnchkulaDocument2 pagesHAREDA PAnchkulaAmit K. YadavNo ratings yet
- KC10 and KC10-FM Manual V1.1Document40 pagesKC10 and KC10-FM Manual V1.1Stoica DanielNo ratings yet
- Consumer Buying Behavior Toeards Milk ProductDocument54 pagesConsumer Buying Behavior Toeards Milk ProductsuyoganuNo ratings yet
- Brown Field TNO 0019 RevDocument2 pagesBrown Field TNO 0019 RevDaniele GouveiaNo ratings yet
- Non-Crystalline Solids: Glasses and Amorphous Solids: Prabhat K. GuptaDocument7 pagesNon-Crystalline Solids: Glasses and Amorphous Solids: Prabhat K. GuptaRafaela Rigoni TeixeiraNo ratings yet
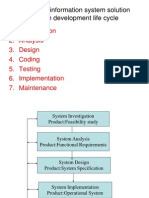
- Developing Information System SolutionDocument42 pagesDeveloping Information System SolutionAbhijeet Mahapatra71% (7)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- HowToBuildAStockStrategy - Portfolio123Document36 pagesHowToBuildAStockStrategy - Portfolio123life_enjoy50% (2)
- Reading W1 SmokingDocument9 pagesReading W1 SmokingLinh Phương TrầnNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)